T4-non-small cell lung cancer invading the thoracic aorta: the role of the hybrid operating room
- PMID: 39975741
- PMCID: PMC11833570
- DOI: 10.21037/jtd-24-1724
T4-non-small cell lung cancer invading the thoracic aorta: the role of the hybrid operating room
Abstract
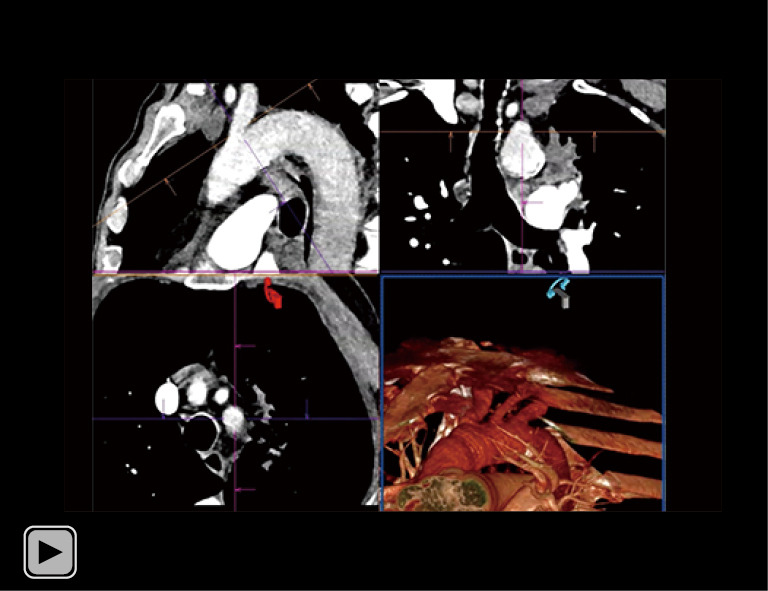
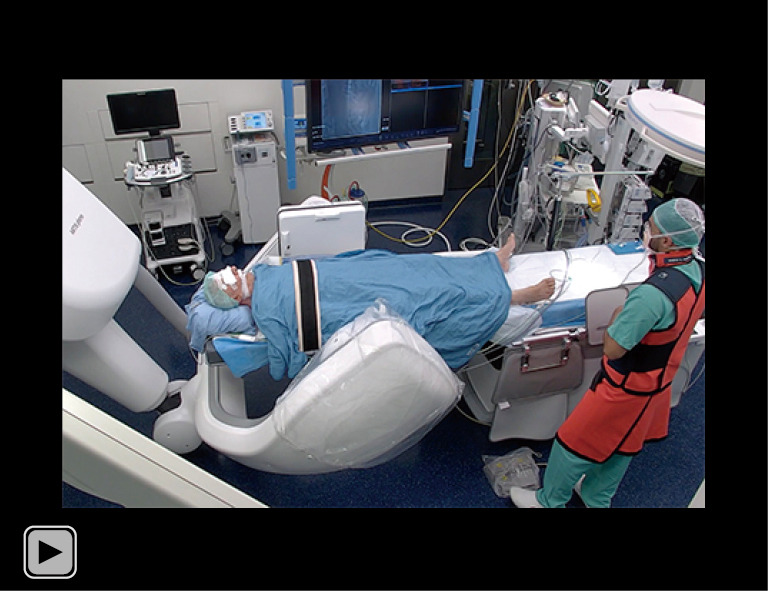
Advanced non-small cell lung cancer (NSCLC) management has become profoundly linked to disease stage and molecular profile. Targeted therapies and immunotherapy have refined treatment options. Developments in minimally invasive surgery and endovascular techniques necessitate reevaluation of T4-NSCLC resectability, especially for T4-NSCLC that invades the thoracic aorta (T4invAo). In cases of suspected aortic invasion in anticipation of surgery, a three-dimensional computed tomography (3D CT) reconstruction is indicated to define the size of the thoracic endoprosthesis that could be used if invasion is confirmed. Preoperative planning meticulously determines the proximal and distal landing zones for the endograft. This crucial step involves carefully considering two key factors: (I) the length of the aortic segment requiring surgical resection during the concomitant thoracic surgical procedure to achieve oncological radicality. This resection encompasses the tumor-infiltrated aortic segment and an additional 2 cm proximal and distal disease-free margin. (II) Further proximal and distal 2-3 cm of the aorta must be added to the planning to ensure adequate endograft apposition to the aortic wall. We propose performing these procedures in a hybrid operating room (HOR) equipped with a C-arm robotic system. In the HOR, the first step involves a video-assisted thoracoscopic surgery diagnostic procedure to confirm the preoperative suspicion of aortic wall invasion. If confirmed, the second step utilizes HOR to place a thoracic endoprosthesis to cover the infiltrated aortic segment. Following patient positioning, image fusion is performed. The preoperative CT reconstruction is matched to these two-dimensional (2D) fluoroscopic images using bony landmarks for real-time 2D-3D image fusion that allows the visualization of the 3D reconstruction overlaid on the live fluoroscopy. Following image fusion, aortography is performed. The stent graft is deployed using standard techniques, with the aid of the fusion image. Following stent-graft deployment, aortography confirms the patency of the side vessels. The third step concludes with en-bloc resection of the lung tumor and the involved aortic wall segment. Thoracic surgeons are encouraged to use HOR in selected cases of T4invAo NSCLC in a "one-stop" approach with the aid of a fusion technique and to actively collaborate with vascular surgeons in planning the endovascular procedure by sharing their oncological know-how.
Keywords: Locally advanced non-small cell lung cancer (locally advanced NSCLC); aortic invasion; hybrid operating room (HOR); thoracic endovascular aortic repair (TEVAR).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-1724/coif). Siemens Healthcare invited F.Z. to speak at the ESTS Meeting 2024 without fees. The other authors have no conflicts of interest to declare.
Figures