

Cancer statistics for African American and Black people, 2025
- PMID: 39976243
- PMCID: PMC11929131
- DOI: 10.3322/caac.21874
Cancer statistics for African American and Black people, 2025
Abstract
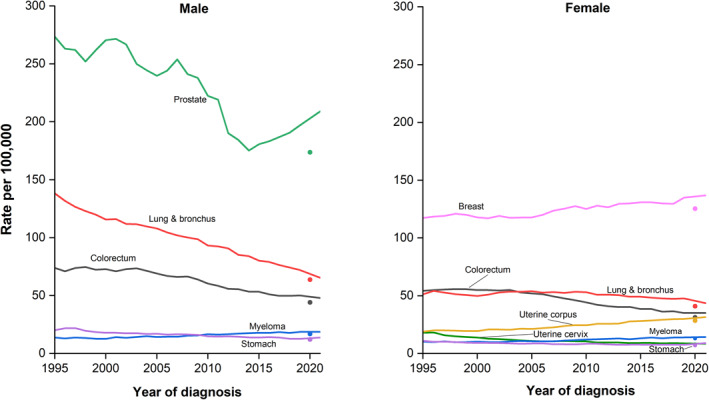
African American and other Black individuals (referred to as Black people in this article) have a disproportionate cancer burden, including the lowest survival of any racial or ethnic group for most cancers. Every 3 years, the American Cancer Society estimates the number of new cancer cases and deaths for Black people in the United States and compiles the most recent data on cancer incidence (herein through 2021), mortality (through 2022), survival, screening, and risk factors using population-based data from the National Cancer Institute and the Centers for Disease Control and Prevention. In 2025, there will be approximately 248,470 new cancer cases and 73,240 cancer deaths among Black people in the United States. Black men have experienced the largest relative decline in cancer mortality from 1991 to 2022 overall (49%) and in almost every 10-year age group, by as much as 65%-67% in the group aged 40-59 years. This progress largely reflects historical reductions in smoking initiation among Black teens, advances in treatment, and earlier detections for some cancers. Nevertheless, during the most recent 5 years, Black men had 16% higher mortality than White men despite just 4% higher incidence, and Black women had 10% higher mortality than White women despite 9% lower incidence. Larger inequalities for mortality than for incidence reflect two-fold higher death rates for prostate, uterine corpus, and stomach cancers and for myeloma, and 40%-50% higher rates for colorectal, breast, cervical, and liver cancers. The causes of ongoing disparities are multifactorial, but largely stem from inequalities in the social determinants of health that trace back to structural racism. Increasing diversity in clinical trials, enhancing provider education, and implementing financial incentives to ensure equitable care across the cancer care continuum would help close these gaps.
Keywords: African Americans; Black people; cancer statistics; incidence; mortality.
© 2025 The Author(s). CA: A Cancer Journal for Clinicians published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
Anatu H. Saka, Angela N. Giaquinto, Jessica Star, Ahmedin Jemal, and Rebecca L. Siegel are employed by the American Cancer Society, which receives grants from private and corporate foundations, including foundations associated with companies in the health sector, for research outside of the submitted work. The authors are not funded by or key personnel for any of these grants, and their salary is solely funded through American Cancer Society funds. The remaining authors disclosed no conflicts of interest.
Figures









References
-
- U.S. Census Bureau . Table DP05. American Community Survey (ACS) Demographic and Housing Estimates. ACS 1‐Year Estimates Data Profiles. U.S. Census Bureau; 2022.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
