

How I do it: surgical techniques for vagus nerve stimulation in pediatric drug-resistant epilepsy
- PMID: 39976670
- PMCID: PMC11842514
- DOI: 10.1007/s00701-025-06432-8
How I do it: surgical techniques for vagus nerve stimulation in pediatric drug-resistant epilepsy
Abstract
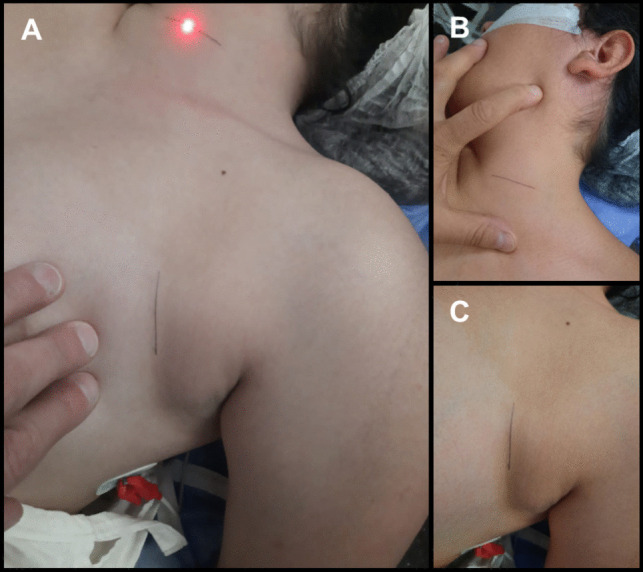
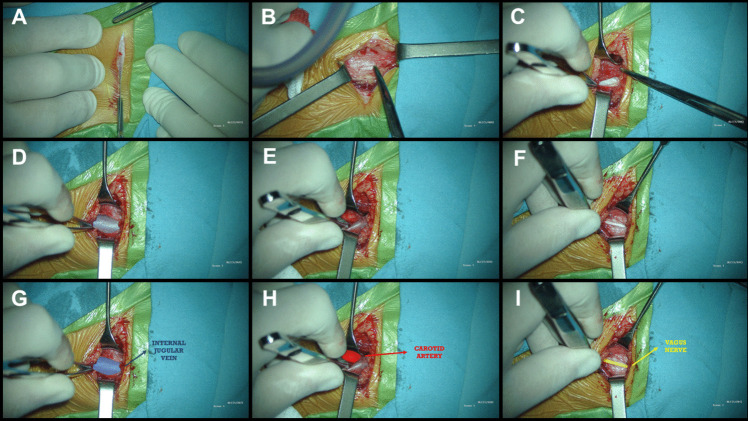
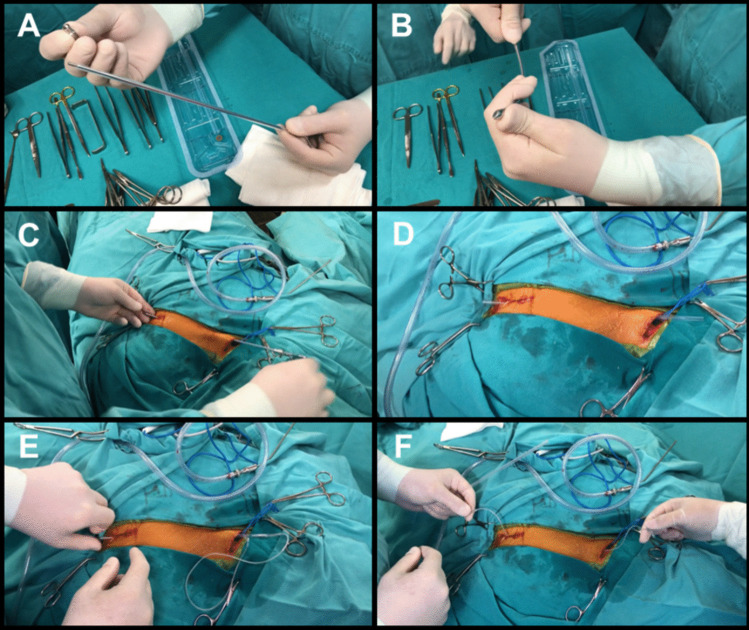
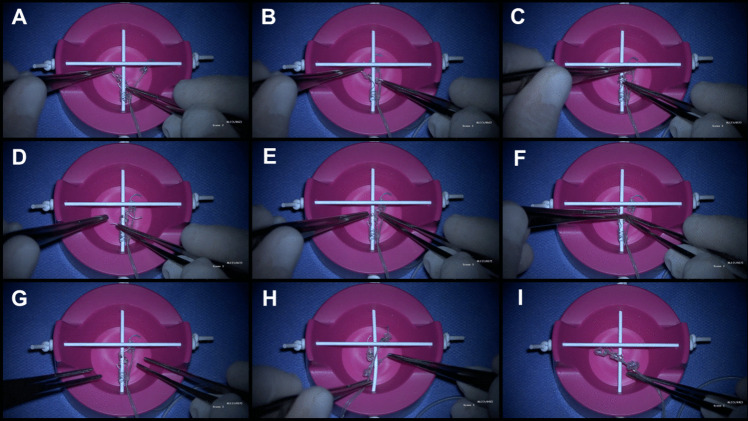
Background: Vagus nerve stimulation (VNS) is a neuromodulatory treatment for refractory epilepsy, involving electrical stimulation of the vagus nerve via a subcutaneously implanted pulse generator.
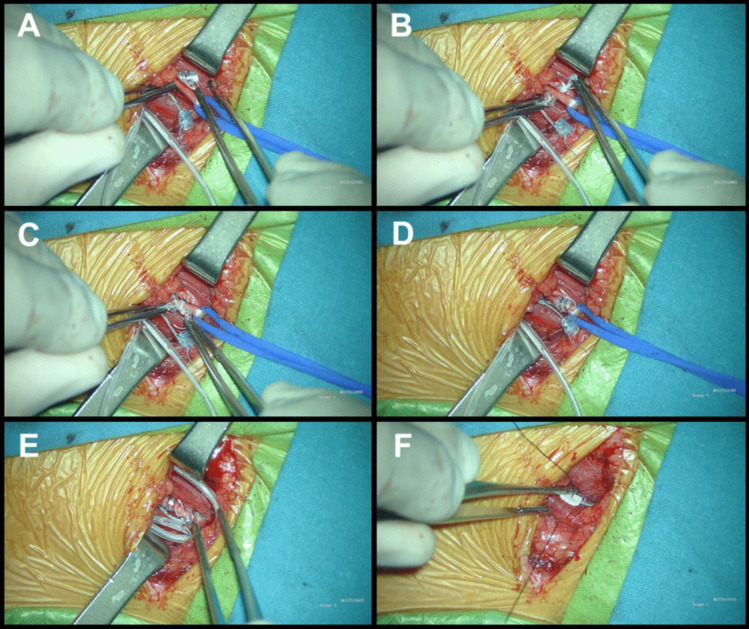
Method: We present a step-by-step description of the VNS implantation technique, incorporating tips and tricks from an epilepsy surgeon with over 20 years of experience (MB).
Conclusion: Proper patient selection, meticulous surgical technique, and comprehensive postoperative care, supported by educational resources such as surgical technique articles, videos, and simulators, are crucial for minimizing complications and optimizing patient outcomes.
Keywords: Drug-resistant epilepsy; Neurosurgery; Surgical technique; Vagus nerve stimulation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: All procedures performed in studies involving human participants were in accordance with the Declaration of Helsinki and adhered to the Good Clinical Practice Guidelines (Resolution 1480/11) of the Argentine Ministry of Health. Furthermore, approval for the protocol was obtained by the Ethics and Research Committee of "Juan P. Garrahan" Pediatric Hospital. Informed consent: Informed consent was obtained from all individual participants included in the study. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Vagus nerve stimulation in epilepsy: Efficiency and safety of outpatient practice.Neurochirurgie. 2020 Aug;66(4):270-274. doi: 10.1016/j.neuchi.2020.04.134. Epub 2020 Jul 2. Neurochirurgie. 2020. PMID: 32623060
-
Vagus nerve stimulator revision in pediatric epilepsy patients: a technical note and case series.Childs Nerv Syst. 2023 Feb;39(2):435-441. doi: 10.1007/s00381-022-05769-0. Epub 2022 Nov 25. Childs Nerv Syst. 2023. PMID: 36434283
-
Vagus nerve stimulation in pediatric patients with drug-resistant epilepsy: a step-by-step video.Neurosurg Focus Video. 2024 Jul 1;11(1):V2. doi: 10.3171/2024.4.FOCVID244. eCollection 2024 Jul. Neurosurg Focus Video. 2024. PMID: 38957417 Free PMC article.
-
[Vagus nerve stimulation for the treatment of refractory epilepsy. State of the art].Neurocirugia (Astur). 2008 Oct;19(5):416-26. Neurocirugia (Astur). 2008. PMID: 18936858 Review. Spanish.
-
Vagus nerve stimulation for drug-resistant epilepsy.Pract Neurol. 2020 May;20(3):189-198. doi: 10.1136/practneurol-2019-002210. Epub 2019 Dec 31. Pract Neurol. 2020. PMID: 31892545 Review.
References
-
- Ansari S, Chaudhri K, Al Moutaery KA (2007) Vagus nerve stimulation: indications and limitations. Acta Neurochir Suppl 97(Pt 2):281–286. 10.1007/978-3-211-33081-4_31 - PubMed
-
- Boon P, De Herdt V, Vonck K, Van Roost D (2007) Clinical experience with vagus nerve stimulation and deep brain stimulation in epilepsy. Acta Neurochir Suppl 97(Pt 2):273–280. 10.1007/978-3-211-33081-4_30 - PubMed
-
- Boon P, Vonck K, Vandekerckhove T et al (1999) Vagus nerve stimulation for medically refractory epilepsy; efficacy and cost-benefit analysis. Acta Neurochir (Wien) 141(5):447–453. 10.1007/s007010050324 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
