

Out-of-Hospital Cardiac Arrest in Apparently Healthy, Young Adults
- PMID: 39976933
- PMCID: PMC12107904
- DOI: 10.1001/jama.2024.27916
Out-of-Hospital Cardiac Arrest in Apparently Healthy, Young Adults
Abstract
Importance: Out-of-hospital cardiac arrest incidence in apparently healthy adults younger than 40 years ranges from 4 to 14 per 100 000 person-years worldwide. Of an estimated 350 000 to 450 000 total annual out-of-hospital cardiac arrests in the US, approximately 10% survive.
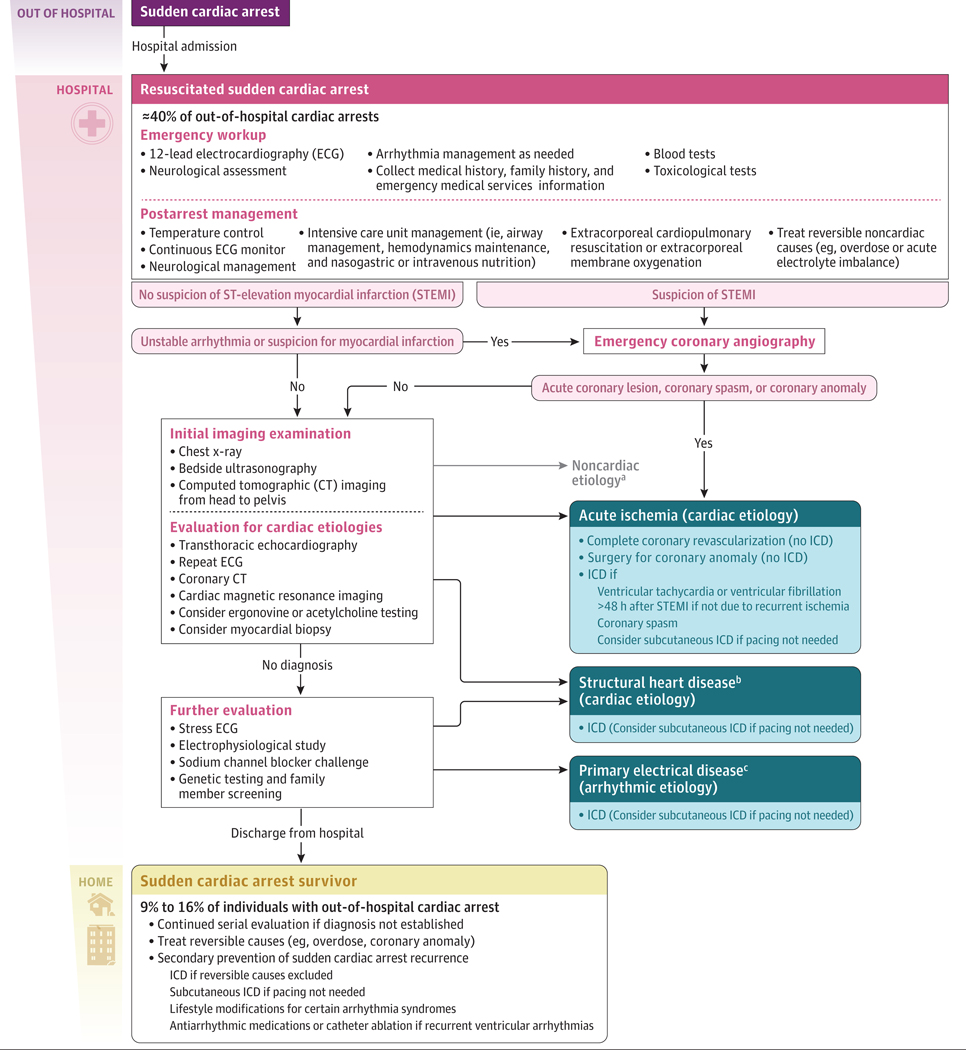
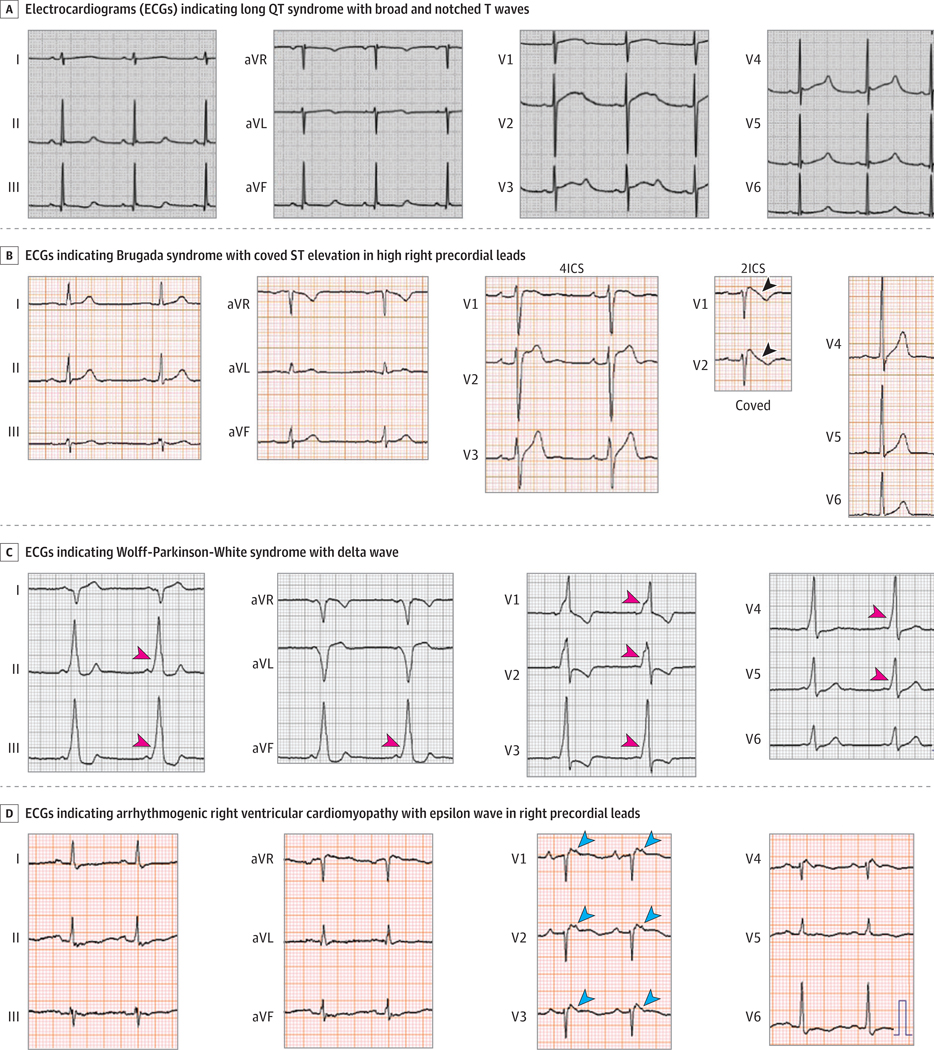
Observations: Among young adults who have had cardiac arrest outside of a hospital, approximately 60% die before reaching a hospital (presumed sudden cardiac death), approximately 40% survive to hospitalization (resuscitated sudden cardiac arrest), and 9% to 16% survive to hospital discharge (sudden cardiac arrest survivor), of whom approximately 90% have a good neurological status (Cerebral Performance Category 1 or 2). Autopsy-based studies demonstrate that 55% to 69% of young adults with presumed sudden cardiac death have underlying cardiac causes, including sudden arrhythmic death syndrome (normal heart by autopsy, most common in athletes) and structural heart disease such as coronary artery disease. Among young adults, noncardiac causes of cardiac arrest outside of a hospital may include drug overdose, pulmonary embolism, subarachnoid hemorrhage, seizure, anaphylaxis, and infection. More than half of young adults with presumed sudden cardiac death had identifiable cardiovascular risk factors such as hypertension and diabetes. Genetic cardiac disease such as long QT syndrome or dilated cardiomyopathy may be found in 2% to 22% of young adult survivors of cardiac arrest outside of the hospital, which is a lower yield than for nonsurvivors (13%-34%) with autopsy-confirmed sudden cardiac death. Persons resuscitated from sudden cardiac arrest should undergo evaluation with a basic metabolic profile and serum troponin; urine toxicology test; electrocardiogram; chest x-ray; head-to-pelvis computed tomography; and bedside ultrasound to assess for pericardial tamponade, aortic dissection, or hemorrhage. Underlying reversible causes, such as ST elevation myocardial infarction, coronary anomaly, and illicit drug or medication overdose (including QT-prolonging medicines) should be treated. If an initial evaluation does not reveal the cause of an out-of-hospital cardiac arrest, transthoracic echocardiography should be performed to screen for structural heart disease (eg, unsuspected cardiomyopathy) or valvular disease (eg, mitral valve prolapse) that can precipitate sudden cardiac death. Defibrillator implant is indicated for young adult sudden cardiac arrest survivors with nonreversible cardiac causes including structural heart disease and arrhythmia syndromes.
Conclusions and relevance: Cardiac arrest in apparently healthy adults younger than 40 years may be due to inherited or acquired cardiac disease or noncardiac causes. Among young adults who have had cardiac arrest outside of a hospital, only 9% to 16% survive to hospital discharge. Sudden cardiac arrest survivors require comprehensive evaluation for underlying causes of cardiac arrest and cardiac defibrillator should be implanted in those with nonreversible cardiac causes of out-of-hospital cardiac arrest.
Conflict of interest statement
Dr Tseng reported receiving grants from the National Heart, Lung, and Blood Institute (R01 HL147035 and R01 HL157247) and the Centers for Disease Control and Prevention (NU58DP007700) during the conduct of the study and holding patent US10959624B2. No other disclosures were reported.
Figures

References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–e621. doi: 10.1161/CIR.0000000000001123 - DOI - PMC - PubMed
-
- McNally B, Robb R, Mehta M, et al. Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ. 2011;60(8):1–19. - PubMed
-
- Jacobs I, Nadkarni V, Bahr J, et al. ; International Liaison Committee on Resuscitation; American Heart Association; European Resuscitation Council; Australian Resuscitation Council; New Zealand Resuscitation Council; Heart and Stroke Foundation of Canada; InterAmerican Heart Foundation; Resuscitation Councils of Southern Africa; ILCOR Task Force on Cardiac Arrest and Cardiopulmonary Resuscitation Outcomes. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation. 2004;110(21):3385–3397. doi: 10.1161/01.CIR.0000147236.85306.15 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
