

Elevated Blood Pressure and Cardiac Mechanics in Children and Adolescents: A Systematic Review and Meta-Analysis
- PMID: 39977013
- PMCID: PMC12080464
- DOI: 10.1093/ajh/hpaf026
Elevated Blood Pressure and Cardiac Mechanics in Children and Adolescents: A Systematic Review and Meta-Analysis
Abstract
Introduction: Evidence on left ventricular (LV) mechanics, assessed by speckle tracking echocardiography (STE), in children and adolescents with elevated blood pressure (BP)/hypertension is scanty.
Aim: The aim of the present meta-analysis was to provide an updated information on LV systolic function phenotyped by global longitudinal strain (GLS) and LV ejection fraction (LVEF) in the setting of pediatric hypertension.
Methods: Systematic searches were conducted across bibliographic databases (Pub-Med, OVID, EMBASE, and Cochrane Library) to identify eligible studies from inception up to 30 November 2024. Studies reporting data on LV mechanics in pediatric hypertension and controls were included. The statistical difference of the echocardiographic variables of interest between groups such as LVEF and GLS was calculated by standardized mean difference (SMD) with 95% confidence interval (CI) using random-effects models.
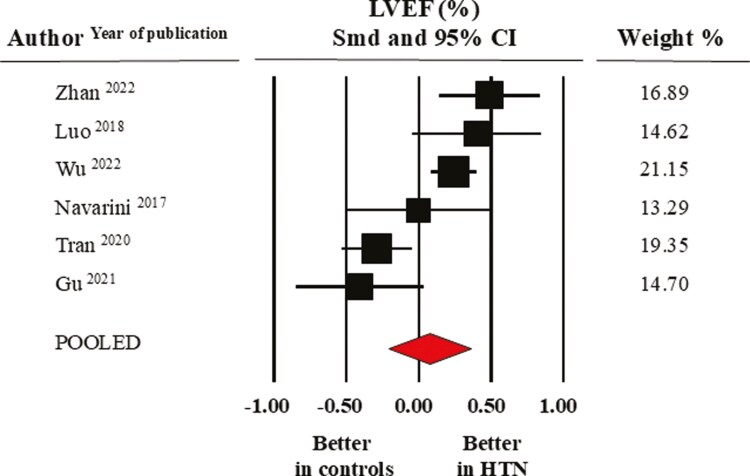
Results: Eight studies including 719 individuals with elevated BP/hypertension and 1,653 age-matched healthy controls were considered for the analysis. Pooled average LVEF values were 72.4 ± 1.6% in the healthy control group and 72.5 ± 1.8% in the elevated BP/hypertensive group (SMD: 0.08 ± 0.15, CI: -0.21/0.36, P = 0.60); the corresponding values of GLS were -19.6 ± 1.1% and 18.5 ± 0.9% (SMD: -0.96 ± 0.25, CI: -1.46/-0.47, P < 0.0001). A parallel impairment of global circumferential strain emerged from pooled data of three studies (SMD: -0.96 ± 0.25, CI: -1.46/-0.47, P < 0.0001).
Conclusions: Our data suggest that LVEF is unable to detect early alterations in systolic function in pediatric hypertension, and the implementation of STE may be highly useful in unmasking systolic dysfunction in this setting.
Keywords: blood pressure; global longitudinal strain; hypertension; left ventricular ejection fraction; pediatric hypertension; systolic function.
© The Author(s) 2025. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Conflict of interest statement
The authors declared no conflict of interest.
Figures





Similar articles
-
Myocardial Mechanics in Acromegaly: A Meta-Analysis of Echocardiographic Studies.High Blood Press Cardiovasc Prev. 2024 Sep;31(5):451-459. doi: 10.1007/s40292-024-00667-9. Epub 2024 Sep 7. High Blood Press Cardiovasc Prev. 2024. PMID: 39242463
-
Myocardial mechanics in anorexia nervosa: a systematic review and meta-analysis of speckle tracking echocardiographic studies.J Cardiovasc Med (Hagerstown). 2024 Oct 1;25(10):740-748. doi: 10.2459/JCM.0000000000001661. Epub 2024 Aug 22. J Cardiovasc Med (Hagerstown). 2024. PMID: 39166392
-
Effect of surgical treatment on left ventricular strain in patients with primary hyperparathyroidism: A meta-analysis of echocardiographic study.Nutr Metab Cardiovasc Dis. 2025 Jul;35(7):103850. doi: 10.1016/j.numecd.2025.103850. Epub 2025 Jan 6. Nutr Metab Cardiovasc Dis. 2025. PMID: 39934044
-
Early Left Ventricular Dysfunction and Non-Dipping: When Ejection Fraction is Not Enough. A Meta-Analysis of Speckle tracking Echocardiography Studies.Am J Hypertens. 2023 Feb 13;36(2):109-119. doi: 10.1093/ajh/hpac110. Am J Hypertens. 2023. PMID: 36169398
-
Obesity and Left Ventricular Mechanics in Children and Adolescents: A Systematic Review and Meta-Analysis.High Blood Press Cardiovasc Prev. 2025 Jul 24. doi: 10.1007/s40292-025-00726-9. Online ahead of print. High Blood Press Cardiovasc Prev. 2025. PMID: 40702258 Review.
References
-
- Takajo D, Przybycien TS, Balakrishnan PL, Natarajan G, Singh GK, Aggarwal S.. Left ventricle hypertrophy and remodeling in children with essential hypertension: does the race matter? Cardiol Young 2024; 34:906–913. - PubMed
-
- Rus RR, Pac M, Obrycki L, Sağsak E, Azukaitis K, Sinha MD, Jankauskiene A, Litwin M; HyperChildNet Working Group 3. Systolic and diastolic left ventricular function in children with primary hypertension: a systematic review and meta-analysis. J Hypertens 2023; 41:51–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
