

Comprehensive geriatric assessment in nonhospitalized settings: An overview of systematic reviews
- PMID: 39979072
- PMCID: PMC11973020
- DOI: 10.1111/ggi.70004
Comprehensive geriatric assessment in nonhospitalized settings: An overview of systematic reviews
Abstract
Aim: Comprehensive geriatric assessment (CGA) is a commonly used intervention for addressing the health needs of older people. Traditionally used for hospital inpatients, there is inconclusive evidence on its effectiveness in other settings. This overview of reviews aims to synthesize the current evidence regarding CGA models, their effectiveness, feasibility and acceptability in nonhospital settings.
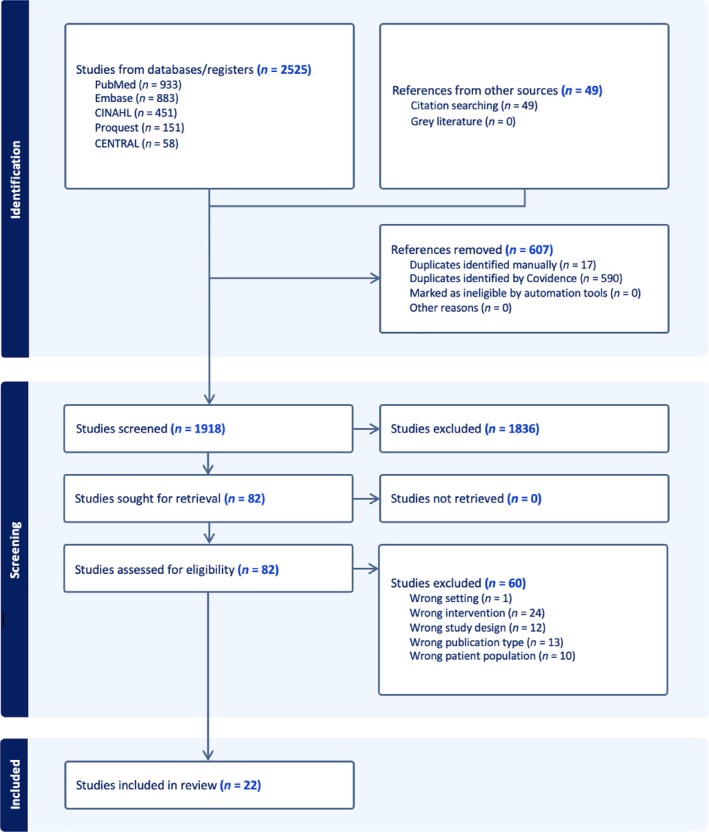
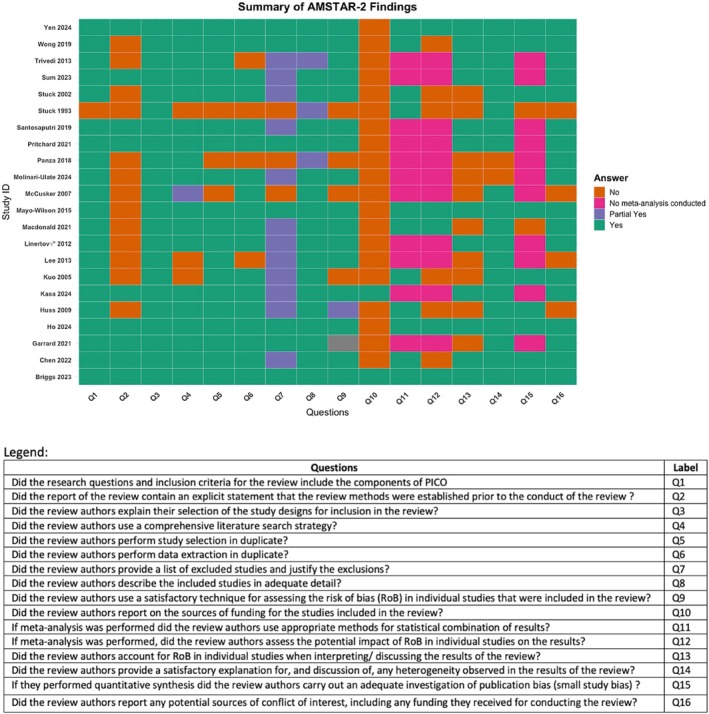
Methodology: The overview included systematic reviews with or without meta-analysis reporting on older adults (≥50 years) undergoing CGA in primary care facilities, outpatient care, community-based programs, long-term care settings and home-based care, excluding narrow high-risk groups or specific disease conditions. MEDLINE, Embase, Cochrane CENTRAL, PsychInfo and CINAHL, were searched up to August 2023, with blinded double screening and data extraction. Review quality was assessed using Assessing the Methodological Quality of Systematic Reviews-2.
Results: Of 2574 identified articles, 22 systematic reviews (478 primary studies, >136 336 participants) met the inclusion criteria. Most reviews were of moderate to good quality, 73% were based in community or home settings, and in 50% of the reviews the participants were aged ≥65 years. They identified diverse CGA models without uniform definition or domains of assessment, most delivered by nurses and multidisciplinary teams, with variation of input duration (6-36 months) and poor reporting of frequency of assessment or follow-up duration. Most reviews found no effect of CGA on rates of admission to hospitals or long-term care facilities, quality of life or function. Of the 10 reviews that reported it as an outcome, only two found that CGA reduced mortality risk by 13% and 14% at longest follow-up. Of the three reviews reporting frailty as an outcome, two showed benefit, with one meta-analysis showing significant reduction in frailty (relative risk, 0.77 [95% CI, 0.64-0.93]). The acceptability of CGA is good among care providers, but limited information was found among patients. Facilitators for implementation identified include preexisting interprofessional working, skilled staff, better informed patients and focus on patient convenience. The evidence was exclusively from high-income countries.
Conclusion: CGA models are highly heterogenous across domains, delivery, dosage and frequency. Most systematic reviews show little to no evidence of benefit of CGA on rates of hospitalization/long-term care admissions, functional ability and quality of life. However, CGA may have a positive effect on frailty and mortality, particularly in relatively vulnerable older people. Strategies to first identify high-risk individuals, followed by CGA, could lead to better outcomes. The lack of evidence on the effectiveness of CGA in low- and middle-income countries, despite the rapid increase in the number and proportion of older adults, means that trials in this area are urgently needed.
Registration: Registered prospectively in the Open Science Framework Registry of reviews (No. ZB69F). Protocol can be accessed at: DOI: https://doi.org/10.17605/OSF.IO/ZB69F. No amendments to the protocol were made. Geriatr Gerontol Int 2025; 25: 491-503.
Keywords: CGA; community‐based CGA; comprehensive geriatric assessment; multidisciplinary geriatric assessment; outpatient CGA.
© 2025 The Author(s). Geriatrics & Gerontology International published by John Wiley & Sons Australia, Ltd on behalf of Japan Geriatrics Society.
Figures
References
-
- Prince MJ, Wu F, Guo Y et al. The burden of disease in older people and implications for health policy and practice. Lancet 2015; 385: 549–562. - PubMed
-
- Pilotto A, Cella A, Pilotto A et al. Three decades of comprehensive geriatric assessment: evidence coming from different healthcare settings and specific clinical conditions. J Am Med Dir Assoc 2017; 18: 192.e1–192.e11. - PubMed
-
- Parker SG, McCue P, Phelps K et al. What is comprehensive geriatric assessment (CGA)? An umbrella review. Age Ageing 2018; 47: 149–155. - PubMed
-
- Stuck AE, Iliffe S. Comprehensive geriatric assessment for older adults. BMJ 2011; 343: d6799. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
