

Efficacy of non-surgical, non-pharmacological treatments for congenital muscular torticollis: a systematic review and meta-analysis
- PMID: 39979901
- PMCID: PMC11844190
- DOI: 10.1186/s12891-025-08407-3
Efficacy of non-surgical, non-pharmacological treatments for congenital muscular torticollis: a systematic review and meta-analysis
Abstract
Background: Congenital Muscular Torticollis (CMT) is the third most common musculoskeletal condition in infancy, and if untreated can lead to significant disability. While a range of conservative treatments are commonly used in the management of CMT, an understanding of their efficacy and safety is limited. This systematic review and meta-analysis, without language or discipline restriction, was conducted to address this knowledge gap.
Methods: Electronic searches of CENTRAL, PubMed, 22 other electronic databases, three trials registers and Google Scholar, were conducted for randomised controlled trials, which examined any non-surgical, non-pharmacological interventions, including but not limited to manual treatments, movement therapy, acupuncture, adjunctive therapies and physical support, in children aged 0 to 5 years with CMT. Two reviewers independently assessed the risk of bias of the included studies using the Cochrane Risk of bias 1 tool, rated their certainty of evidence using grading of recommendations assessment, development and evaluation (GRADE) framework, and performed random-effects meta-analyses.
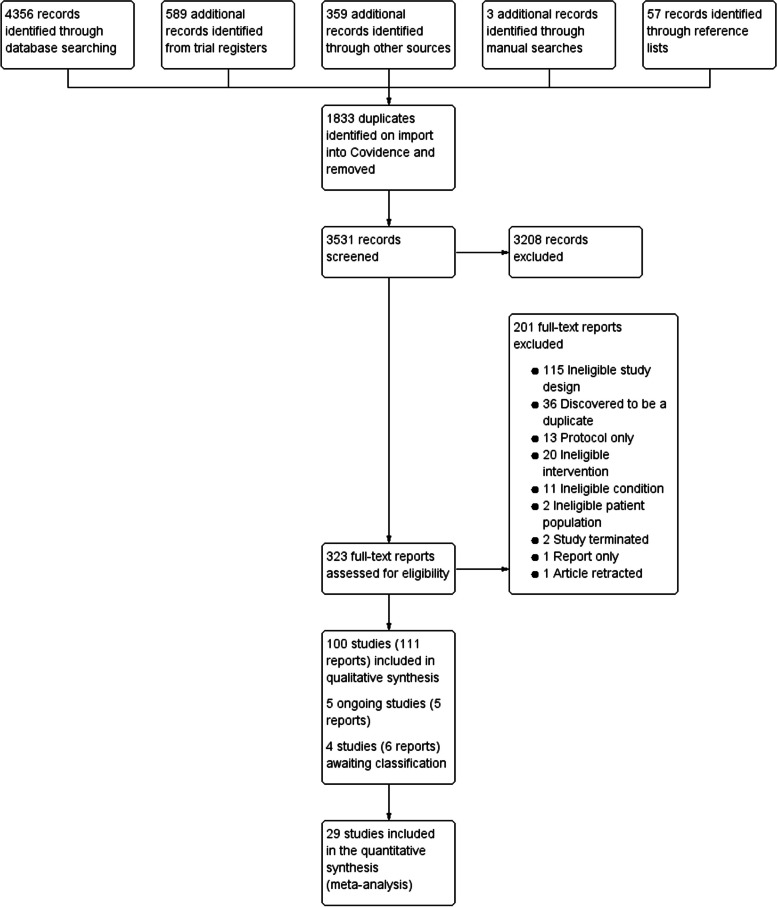
Results: One hundred studies (80 from China) involving 8125 participants published between 1990 and 2023 were included. Adding manual therapy to an active control resulted in short-term improvements in passive cervical rotation (odds ratio (OR) 9.79, 95%CI 4.26,22.50), passive cervical lateroflexion (OR 2.66, 95%CI 1.17,6.04), active cervical rotation (OR 3.94, 95%CI 1.08,14.35), symmetric head posture (OR 4.55, 95%CI 2.57,8.05), sternocleidomastoid tumour thickness (mean difference (MD) -2.12 mm, 95%CI -2.98,-1.26) and development of symmetrical movement (standardised MD -0.70, 95%CI -0.95,-0.45). The addition of an electrophysical agent to an active control reduced sternocleidomastoid tumour thickness (MD -2.03 mm, 95%CI -2.67,-1.39) and optimised Tuina reduced tumour thickness more than traditional Tuina (MD -1.20 mm, 95%CI -1.80,-0.59). Adverse events were uncommon but poorly reported, with 71 (71%) of studies providing no data. Study heterogeneity limited pooling of data for meta-analysis, and there was very low to low certainty evidence for all results, due to high risk of bias, small sample sizes and study heterogeneity.
Conclusions: This review found that non-surgical, non-pharmacological treatments may be effective for CMT, but the certainty of evidence is very low to low. These findings are important in informing clinical guidelines and management for CMT and highlight an urgent need for large definitive trials that address the limitations of current studies.
Protocol registration: Cochrane Database of Systematic Reviews (No.: CD012987).
Keywords: Conservative treatment; Electrophysical agents; Infant; Manual therapy; Safety; Traditional Chinese Massage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




References
-
- Stellwagen L, Hubbard E, Chambers C, Jones KL. Torticollis, facial asymmetry and plagiocephaly in normal newborns. Arch Dis Child. 2008;93(10):827–31. - PubMed
-
- Golden KA, Beals SP, Littlefield TR, Pomatto JK. Sternocleidomastoid imbalance versus congenital muscular torticollis: their relationship to positional plagiocephaly. Cleft Palate Craniofac J. 1999;36(3):256–61. - PubMed
-
- Persing J, James H, Swanson J, Kattwinkel J. Prevention and management of positional skull deformities in infants. Pediatrics. 2003;112(1):199–203. - PubMed
-
- De Chalain TM, Park S. Torticollis associated with positional plagiocephaly: a growing epidemic. Journal of Craniofacial Surgery. 2005;16(3):411–8. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Miscellaneous
