

A multi-level implementation strategy to increase adoption of chiropractic care for low back pain in primary care clinics: a randomized stepped-wedge pilot study protocol
- PMID: 39979943
- PMCID: PMC11844171
- DOI: 10.1186/s12998-024-00565-w
A multi-level implementation strategy to increase adoption of chiropractic care for low back pain in primary care clinics: a randomized stepped-wedge pilot study protocol
Abstract
Introduction: Limited adoption of first line treatments for low back pain (LBP) in primary care settings may contribute to an overreliance on pain medications by primary care providers (PCPs). While chiropractic care typically includes recommended nonpharmacologic approaches (e.g., manual therapy, exercise instruction, advice on self-care), implementation strategies to increase adoption of chiropractic care for LBP in primary care clinics are understudied, particularly in underserved communities.
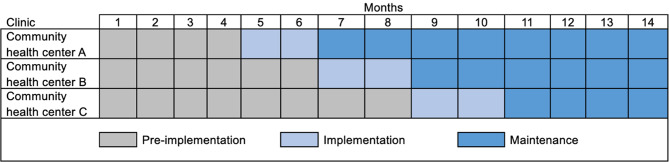
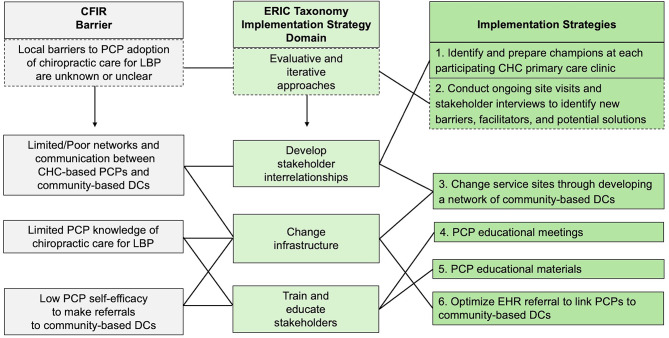
Methods: We will use a stepped-wedge cluster randomized controlled pilot trial design to evaluate the feasibility of a multi-level implementation strategy to increase adoption of chiropractic care for LBP in primary care clinics at community health centers. Key barriers and facilitators identified by site champions and other key stakeholders will help us to develop and tailor implementation strategies including educational materials and meetings, developing a network of local chiropractors, and modifying the electronic health record to facilitate referrals. Three primary care clinics will be randomized to receive the implementation strategy first, second, or third over a fourteen-month study period. At our first clinic, we will have a four-month pre-implementation period, a two-month implementation deployment period, and a subsequent eight-month follow-up period. We will stagger the start of our implementation strategy, beginning in a new clinic every two months. We will evaluate the proportion of patients with LBP who receive a referral to chiropractic care in the first 21 days after their index visit with PCP. We will also evaluate adoption of other guideline concordant care (e.g., other nonpharmacologic treatments) and non-guideline concordant care (e.g., opioids, imaging) over the study period.
Discussion: LBP is currently the leading cause of disability worldwide. While there are several treatment options available for individuals with LBP, patients in underserved populations do not often access recommended nonpharmacologic treatment options such as chiropractic care. The results from this study will inform the development of practical implementation strategies that may improve access to chiropractic care for LBP in the primary care context. Furthermore, results may also inform policy changes needed to expand access to chiropractic care in underserved communities. CLINTRIALS.GOV NCT#: NCT06104605.
Keywords: Chiropractic care; Chronic pain; Community health center; Low back pain; Nonpharmacologic treatment; Primary care.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Boston University Medical Campus IRB. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
