

Impact of enzyme replacement therapy and migalastat on disease progression in females with fabry disease
- PMID: 39980015
- PMCID: PMC11843741
- DOI: 10.1186/s13023-025-03600-y
Impact of enzyme replacement therapy and migalastat on disease progression in females with fabry disease
Abstract
Aim: The aim of our multicenter study was to investigate the safety and efficacy of enzyme replacement therapy (ERT) and chaperone therapy on the disease progression in female Fabry disease (FD) patients and to compare the individual treatment regimens.
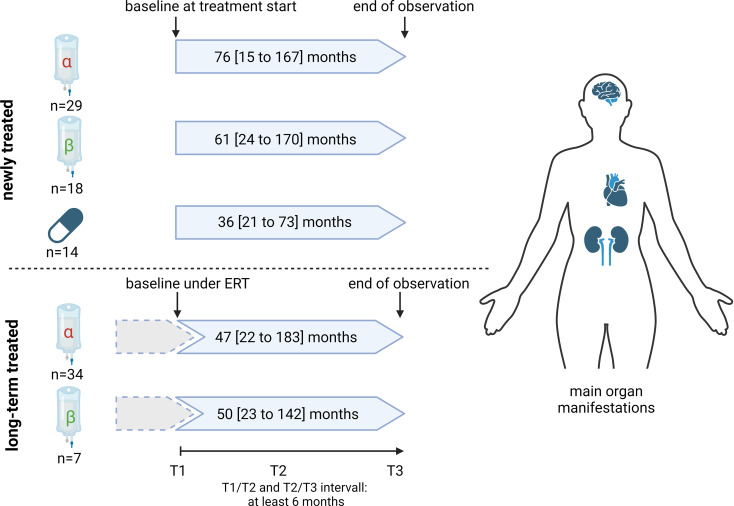
Methods: Data from 3 consecutive visits of 102 female FD patients from 6 Fabry centers were retrospectively analyzed. According to their FD-specific treatment, patients were separated in 5 groups: Newly agalsidase-beta- [n = 18], agalsidase-alfa- [n = 29] and migalastat-[n = 14] treated patients, and long-term agalsidase-beta- [n = 7] and agalsidase-alfa-[n = 34] treated patients. Clinical presentation and laboratory data, including plasma lyso-Gb3 levels were assessed.
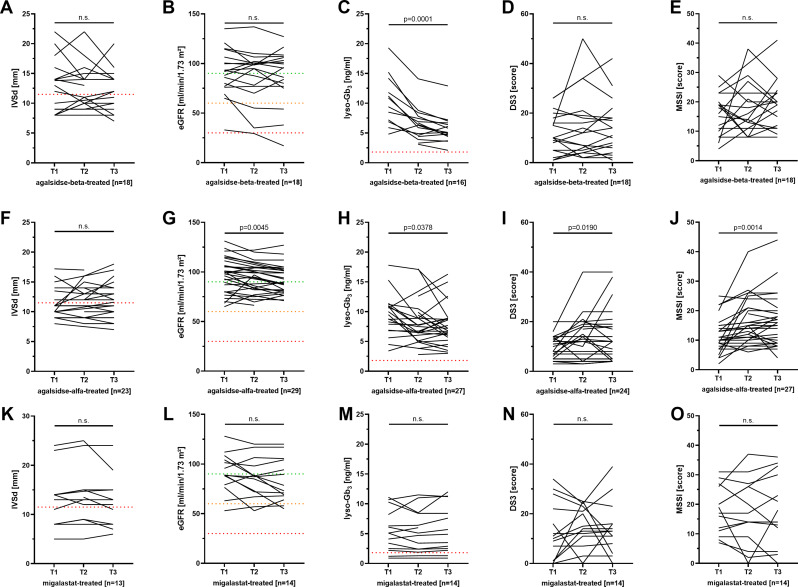
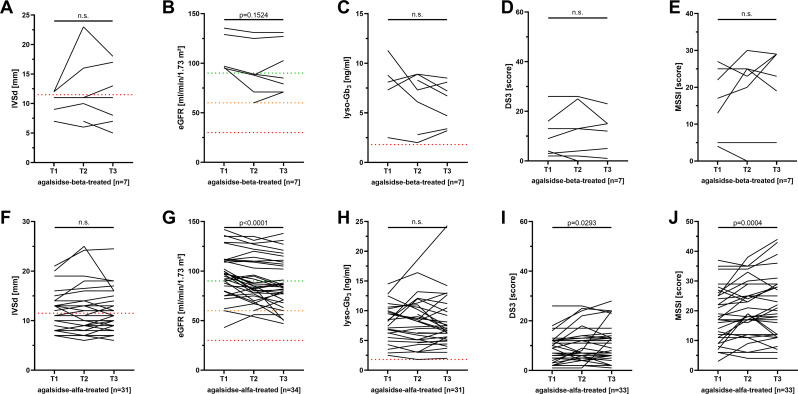
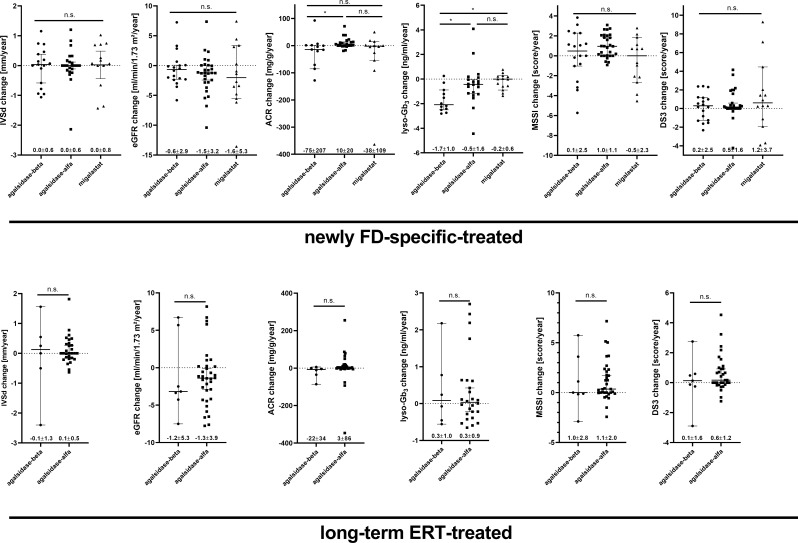
Results: Treatment with agalsidase-beta, agalsidase-alfa, and migalastat was safe and severe adverse events were rare. Newly and long-term-treated patients presented a stable disease course over time. None of the patients required hospitalization due to cardiac events. Overall septum thickness remained stable in all groups (p > 0.05). Estimated glomerular filtration rate (eGFR) only slightly decreased in patients treated with agalsidase-alfa [newly- and long-term-treated: -1.5 ± 3.2 and - 1.3 ± 3.9 ml/min/1.73 m²/year; p = 0.0056 and p = 0.0187, respectively] but the decrease was in the range of natural eGFR decline. eGFRs in agalsidase-beta and migalastat-treated patients were stable. No clinically relevant differences concerning treatment efficacy between agalasidase-beta, agalsidase-alfa, and migalastat were detected.
Conclusion: We conclude that treatment of females with agalsidase-beta, agalsidase-alfa, and migalastat was safe. Independent of the chosen treatment regimen, nearly all patients presented with a stable disease course over time. In our cohort, a comparison of therapy efficacies showed no relevant clinical differences between the groups.
Keywords: Disease progression; Enzyme replacement therapy; Fabry disease; Females; Migalastat.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All investigations were performed after approval by the respective ethics committees of the participating centers (project number: 2016-401-f-S; 2011-347-f). Consent for publication: Written informed consent for molecular analysis and publication was obtained from patients. Competing interests: ML received speaker honoraria, travel funding and research grants from Amicus Therapeutics, Sanofi, Chiesi, Sumitomo Pharma, and Takeda. AN received speaker honoraria and research grants from Amicus, Takeda, and Sanofi. AFK received speaker honoraria and/or travel grants from Amicus Therapeutics, Biomarin, Orphazyme, Sanofi, and Takeda. NMM is a consultant for Amicus Therapeutics, Biomarin, Chiesi, JCR, Sanofi, Takeda, and Orphazyme and received speakers honoraria and travel grants from Amicus Therapeutics, Biomarin, Chiesi, Sanofi, and Takeda. JK received speaker honoraria and/or travel funding from Amicus Therapeutics, Sanofi, Chiesi, Novartis, and Takeda. CK received speaker honoraria and travel support from Amicus Therapeutics, Chiesi, Eleva, Sanofi, and Takeda. MC received speaker honoraria/travel grants from Takeda, Amicus Therapeutics, Idorsia, and Alexion. EB received research grants and speaker honoraria from Sanofi, Takeda, Chiesi, Eleva, and Amicus Therapeutics.
Figures
References
-
- Zarate YA, Hopkin RJ. Fabry’s disease. Lancet. 2008;372:1427–35. - PubMed
-
- Germain DP, Arad M, Burlina A, Elliott PM, Falissard B, Feldt-Rasmussen U, Hilz MJ, Hughes DA, Ortiz A, Wanner C, Weidemann F, Spada M. The effect of enzyme replacement therapy on clinical outcomes in female patients with fabry disease - A systematic literature review by a European panel of experts. Mol Genet Metab. 2019;126:224–35. - PubMed
-
- Ortiz A, Germain DP, Desnick RJ, Politei J, Mauer M, Burlina A, Eng C, Hopkin RJ, Laney D, Linhart A, Waldek S, Wallace E, Weidemann F, Wilcox WR. Fabry disease revisited: management and treatment recommendations for adult patients. Mol Genet Metab. 2018;123:416–27. - PubMed
-
- Fuller M, Mellett N, Hein LK, Brooks DA, Meikle PJ. Absence of α-galactosidase cross-correction in fabry heterozygote cultured skin fibroblasts. Mol Genet Metab. 2015;114:268–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
