

Global burden of metabolic dysfunction-associated steatotic liver disease, 2010 to 2021
- PMID: 39980749
- PMCID: PMC11840544
- DOI: 10.1016/j.jhepr.2024.101271
Global burden of metabolic dysfunction-associated steatotic liver disease, 2010 to 2021
Abstract
Background & aims: This study used the Global Burden of Disease data (2010-2021) to analyze the rates and trends of point prevalence, annual incidence, and years lived with disability (YLDs) for metabolic dysfunction-associated steatotic liver disease (MASLD) in 204 countries.
Methods: Total numbers and age-standardized rates per 100,000 population for MASLD prevalence, annual incidence, and YLDs were compared across regions and countries by age, sex, and sociodemographic index (SDI). Smoothing spline models were used to evaluate the relationship between the burden of MASLD and SDI. Estimates were reported with uncertainty intervals (UI).
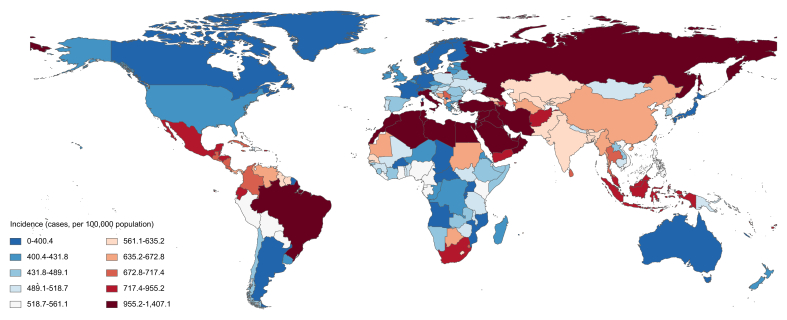
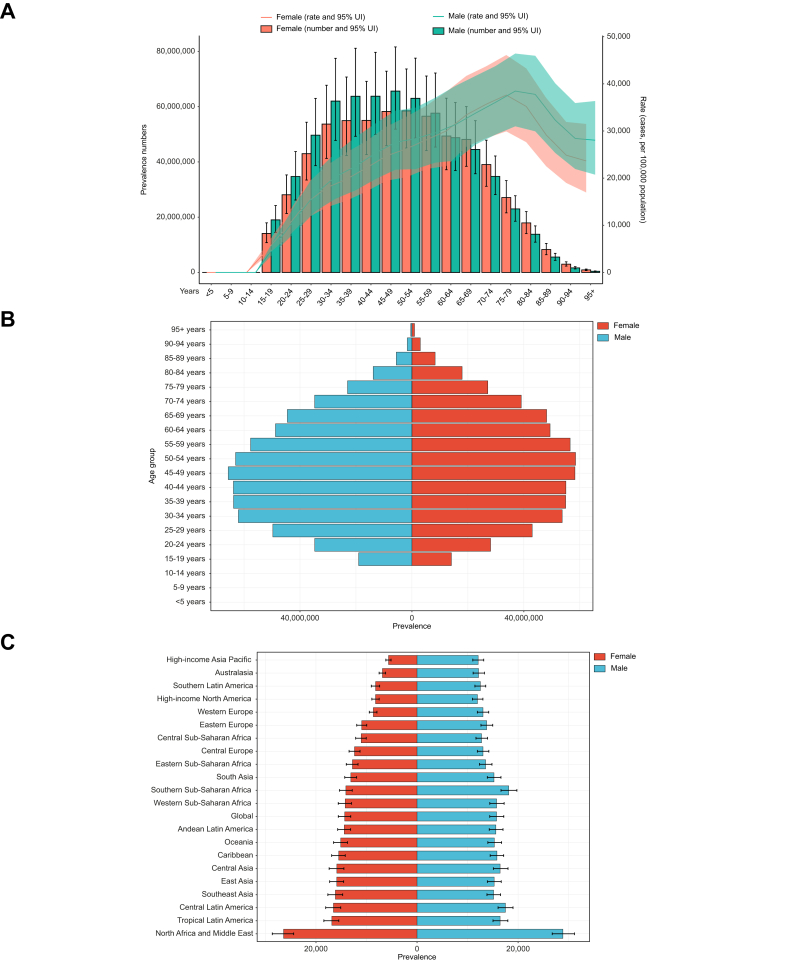
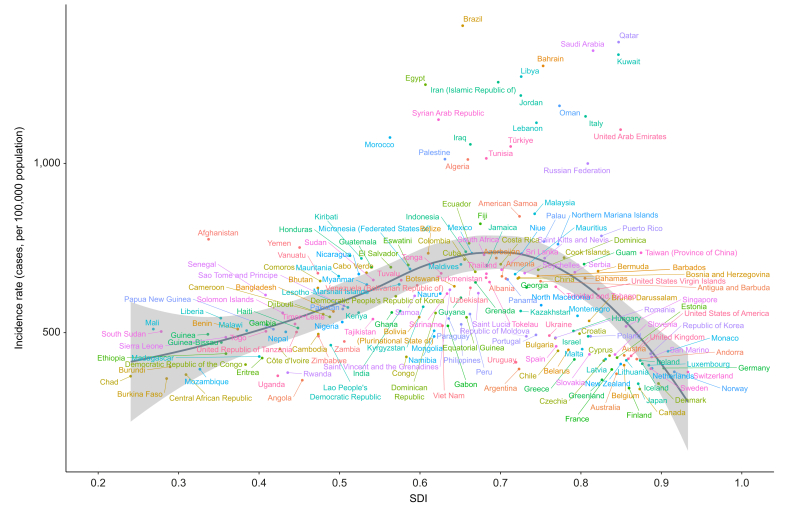
Results: Globally, in 2021, the age-standardized rates per 100,000 population of point prevalence of MASLD were 15,018.1 cases (95% UI 13,756.5-16,361.4), annual incidence rates were 608.5 cases (598.8-617.7), and YLDs were 0.5 (0.3-0.8) years. MASLD point prevalence was higher in men than women (15,731.4 vs. 14,310.6 cases per 100,000 population). Prevalence peaked at ages 45-49 for men and 50-54 for women. Kuwait (32,312.2 cases per 100,000 people; 95% UI: 29,947.1-34,839.0), Egypt (31,668.8 cases per 100,000 people; 95% UI: 29,272.5-34,224.7), and Qatar (31,327.5 cases per 100,000 people; 95% UI: 29,078.5-33,790.9) had the highest prevalence rates in 2021. The largest increases in age-standardized point prevalence estimates from 2010 to 2021 were in China (16.9%, 95% UI 14.7%-18.9%), Sudan (13.3%, 95% UI 9.8%-16.7%) and India (13.2%, 95% UI 12.0%-14.4%). MASLD incidence varied with SDI, peaking at moderate SDI levels.
Conclusions: MASLD is a global health concern, with the highest prevalence reported in Kuwait, Egypt, and Qatar. Raising awareness about risk factors and prevention is essential in every country, especially in China, Sudan and India, where disease incidence and prevalence are rapidly increasing.
Impact and implications: This research provides a comprehensive analysis of the global burden of MASLD, highlighting its rising prevalence and incidence, particularly in countries with varying sociodemographic indices. The findings are significant for both clinicians and policymakers, as they offer critical insights into the regional disparities in MASLD burden, which can inform targeted prevention and intervention strategies. However, the study's reliance on modeling and available data suggests cautious interpretation, and further research is needed to validate these findings in clinical and real-world settings.
Keywords: Epidemiology; Metabolic dysfunction-associated fatty liver disease; Metabolic dysfunction-associated steatotic liver disease; Non-alcoholic fatty liver disease.
© 2024 The Author(s).
Conflict of interest statement
CDB has received grant support from Echosens. YY is a consultant to Zydus and Novo Nordisk. WK reports grants from Glaxo-SmithKline, Gilead, Novartis, Pfizer, Roche, Springbank, Ildong, Galmed, Dicerna, Enyo, Hanmi, Novo Nordisk, and KOBIOLABS; consulting fees from Boehringer Ingelheim, Novo Nordisk, Standigm, Daewoong, TSD Life Sciences Ildong, Olix Pharma, HK Inoen, and KOBIOLABS; honoraria for lectures from Ildong, Samil, and Novo Nordisk, and owns stocks in KOBIOLABS and Lepidyne and he is the founder of Remedygen. GS reports honoraria from Merck, Gilead, AbbVie, Novonordisk, and Pfizer, and unrestricted research funding from Theratecnologies Inc. VW-SW reports grants from Gilead Sciences; consulting fees from AbbVie, Boehringer Ingelheim, Echosens, Gilead Sciences, Intercept, Inventiva, Novo Nordisk, Pfizer, TARGET PharmaSolutions; honoraria for lectures from Abbott, AbbVie, Gilead Sciences, Novo Nordisk and he is Chairman of Subspecialty Board of Gastroenterology and Hepatology, Hong Kong College of Physicians and Co-founder of Illuminatio Medical Technology Limited. JB reported receiving grants and personal fees from Echosens. W-KC is a consultant or advisory board member for Abbott, Roche, AbbVie, Boehringer Ingelheim and Novo Nordisk; and a speaker for Abbott, Novo Nordisk, Echosens, Viatris and Hisky Medical. JDR received consultancy fees from Falk, Gilead, Pfizer and a speaker honorarium from Takeda. LV reports consulting fees from Gilead, Pfizer, Astra Zeneca, Novo Nordisk, Intercept pharmaceuticals, Diatech Pharmacogenetics, IONIS, and Viatris; honoraria from MSD, Gilead, AlfaSigma, AbbVie, and Resalis, and grants from Gilead. JMS serves as a consultant for Akero, Alentis Therapeutics, Astra Zeneca, Apollo Endosurgery, Boehringer Ingelheim, GSK, Ipsen, Inventiva Pharma, Madrigal, MSD, Northsea Therapeutics, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi, and Siemens Healthineers. He has received research funding from Gilead Sciences, Boehringer Ingelheim, and Siemens Healthcare GmbH. He holds stock options in AGED diagnostics and Hepta Bio. He has also received speaker honorarium from Gilead Sciences, Advanz, Echosens, MedPublico GmbH. MR-G reported receiving personal fees from Echosens. SUK reported personal fees from Gilead Sciences, GSK, Bayer, Eisai, AbbVie, Echosens, MSD, Bristol-Myers Squibb, AstraZeneca, and grants from AbbVie, Bristol-Myers Squibb, and Gilead Sciences. PNN reported receiving grants from Novo Nordisk, advisory board and personal consulting fees, honoraria for lectures and travel expenses from Novo Nordisk, personal consulting and advisory board fees from Boehringer Ingelheim, Gilead, Intercept, Poxel Pharmaceuticals, Bristol-Myers Squibb, Pfizer, MSD, Sun Pharma, Eli Lilly, Madrigal, GSK, and nonfinancial support for educational events from AiCME. AS reported receiving grants from Intercept, Merck, personal consulting fees from Gilead, Pfizer, Genentech, ALnylam, Regeneron, Zydus, LG chem, Hanmi, Madrigal, Path AI, and 89 Bio, grants and personal consulting fees from Eli Lilly, Novo Nordisk, Boehringer Ingelheim, Novartis, and Histoindex, and stock options from Genfit, Tiziana, Durect, Inversago, and Galmed. LAA reports consulting fees from Novo Nordisk, Pfizer, Gilead, and CSL Behring. HH reported personal fees from AstraZeneca, Bristol-Myers Squibb, MSD, Novo Nordisk, Boehringer Ingelheim, KOWA, and GW Phara outside the submitted work, and grants from AstraZeneca, Echosens, Gilead Sciences, Intercept, MSD, Novo Nordisk, and Pfizer outside the submitted work. JG serves on Advisory Boards and receives honoraria for talks from Novo Nordisk, Astra Zeneca, Roche, BMS, Pfizer, Cincera, Pharmaxis, Gilead, AbbVie, and Boehringer Ingelheim. M-HZ has received honoraria for lectures from AstraZeneca, Hisky Medical Technologies, and Novo Nordisk, and consulting fees from Boehringer Ingelheim. No other disclosures were reported. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
-
- Rinella M.E., Lazarus J.V., Ratziu V., et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78:1966–1986. - PubMed
-
- Li Q.-Q., Xiong Y.-T., Wang D., et al. Metabolic syndrome is associated with significant hepatic fibrosis and steatosis in patients with nonalcoholic steatohepatitis. iLIVER. 2024;3
-
- Feng G., Fan Y.-F., Li R.-X., et al. Unraveling the epidemiology of metabolic dysfunction-associated liver cancer: insights from mixed etiologies, regional variations, and gender disparities. iLIVER. 2024 doi: 10.1016/j.iliver.2024.100113. - DOI
-
- Huang H., Liu Z., Xu M., et al. Global burden trends of MAFLD-related liver cancer from 1990 to 2019. Portal Hypertens Cirrhosis. 2023;2:157–164.
