

Placental growth factor modulates endothelial NO production and exacerbates experimental hepatopulmonary syndrome
- PMID: 39980753
- PMCID: PMC11840504
- DOI: 10.1016/j.jhepr.2024.101297
Placental growth factor modulates endothelial NO production and exacerbates experimental hepatopulmonary syndrome
Abstract
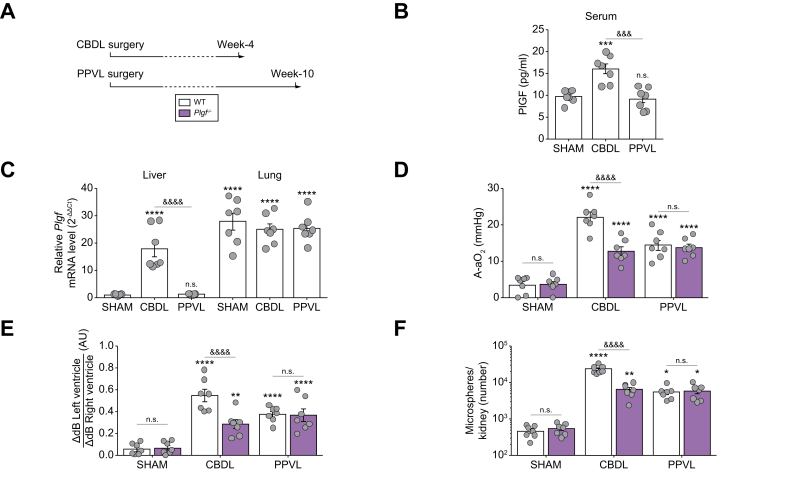
Background & aims: Hepatopulmonary syndrome (HPS) results from portal hypertension, with or without cirrhosis, and is marked by pulmonary vascular dilations leading to severe hypoxemia. Although placental growth factor (PlGF) is important for vascular growth and endothelial function, its role in HPS is unclear. This study investigated the involvement of PlGF in experimental models of HPS and in patients.
Methods: Circulating PlGF levels were measured in 64 controls and 137 patients with liver disease, with or without HPS. Two rat models, common bile duct ligation (CBDL) and long-term partial portal vein ligation (PPVL), were used. Plgf-knockout (Plgf -/-) rats were generated using CRISPR-Cas9. Lung RNA-sequencing analysis was performed in the CBDL model. The effects of PlGF on endothelial nitric oxide synthase (eNOS) activity in human pulmonary microvascular endothelial cells were also investigated.
Results: Circulating PlGF levels were significantly higher in patients with cirrhosis compared with healthy controls (29.4 ± 1.2 vs. 20.2 ± 0.8 pg/ml, p <0.0001), but no difference were found between patients with and without HPS. PlGF levels were not elevated in patients with extrahepatic portal hypertension. In Plgf -/- rats, there was a protective effect against CBDL-induced HPS, whereas PPVL-induced HPS severity remained unchanged. RNA sequencing coupled with ingenuity pathway analysis identified significant interactions between PlGF and pulmonary eNOS activity. Following CBDL, Plgf -/- rats showed decreased pulmonary eNOS activity and reduced circulating nitric oxide metabolites. In vitro, PlGF stimulation enhanced eNOS activity in human pulmonary microvascular endothelial cells, whereas PlGF knockdown led to a decrease.
Conclusions: These findings indicate that PlGF aggravates cirrhosis-induced HPS through modulation of pulmonary eNOS activity, and is not involved in HPS from extrahepatic portal hypertension.
Impact and implications: This study identified PlGF as a significant contributor to the exacerbation of HPS associated with cirrhosis, through its regulation of pulmonary nitric oxide production. Our findings demonstrated that PlGF deficiency mitigates the severity of both cirrhosis and HPS in the CBDL model, highlighting its potential as a therapeutic target in cirrhosis-induced HPS. Notably, this protective effect was absent in the PPVL model, which induces HPS associated with portal hypertension without cirrhosis. These results open avenues for novel pharmacological interventions aiming to improve outcomes for patients with cirrhosis-induced HPS.
Keywords: Common bile duct ligation; Hypoxemia; Intrapulmonary vascular dilations; Liver cirrhosis; Partial portal vein ligation; Portal hypertension; Pulmonary endothelial dysfunction; VEGF.
© 2024 The Author(s).
Conflict of interest statement
Over the past 3 years, C.G. reports grants from Acceleron Pharma, a wholly owned subsidiary of Merck & Co., Inc., MSD, Corteria Pharmaceuticals, Structure therapeutics (ex ShouTi), Diagonal Therapeutics, and Gossamer, outside the submitted work. M.H. reports grants and personal fees from Acceleron, Aerovate, Altavant, AOP Orphan, Bayer, Chiesi, Ferrer, Janssen, Merck, MorphogenIX, and United Therapeutics, outside the submitted work. L.S. reports personal fees from Bayer, MSD, and Janssen, and grants from Acceleron, Janssen, MSD, outside the submitted work. All the other authors declare no conflict of interest regarding the publication of this article. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures




References
-
- Younis I., Sarwar S., Butt Z., et al. Clinical characteristics, predictors, and survival among patients with hepatopulmonary syndrome. Ann Hepatol. 2015;14:354–360. - PubMed
-
- Schenk P., Schöniger-Hekele M., Fuhrmann V., et al. Prognostic significance of the hepatopulmonary syndrome in patients with cirrhosis. Gastroenterology. 2003;125:1042–1052. - PubMed
LinkOut - more resources
Full Text Sources
