

Spot Versus 24-Hour Urine Osmolality Measurement in Autosomal Dominant Polycystic Kidney Disease: A Diagnostic Test Study
- PMID: 39980937
- PMCID: PMC11840182
- DOI: 10.1016/j.xkme.2025.100965
Spot Versus 24-Hour Urine Osmolality Measurement in Autosomal Dominant Polycystic Kidney Disease: A Diagnostic Test Study
Abstract
Rationale & objective: Arginine vasopressin (AVP) is an established driver of cyst growth in autosomal dominant polycystic kidney disease (ADPKD). Urine osmolality (osm) measures are surrogate markers of AVP activity. Both 24-hour and spot urine samples are used as indicators of AVP suppression. The agreement between these 2 measurements remains unclear.
Study design: A retrospective cohort study.
Setting & study population: Three hundred and forty-nine patients with ADPKD with 839 urine samples from a tertiary care center.
Selection criteria for study: Patients with ADPKD with records of spot and 24-hour urine measurements.
Data extraction: Consecutive patients' data from January 2018 to March 2023 were extracted from the quality assurance database of The Ottawa Hospital Cystic Kidney Disease Clinic.
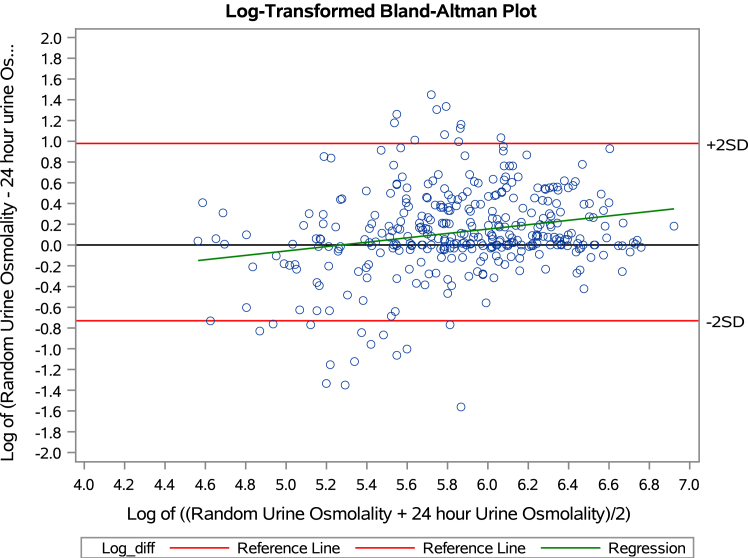
Analytical approach: Discordance assessed at target urine osmolality of 250 and 270 mmol/kg. Agreement assessed by Bland-Altman plots. The percentage of patients with difference in osmolality between the 2 measures for cutoff points of > 50, > 100, >150, and > 200 mmol/kg was calculated.
Results: The mean 24-hour urine osm was 364 mmol/kg, and the mean spot urine osm was 424 mosm/kg. Mean age of 46 years, 52% females, and 47 (13.5%) were on tolvaptan. Overall, in comparing spot urine osm to 24-hour urine osm, the discordance at 250 and 270 mmol/kg was 24% with poor agreement on Bland-Altman plots. The differences between the 2 measures at varying cutoff points were 53.9% at 50 mmol/kg, 35.8% at 100 mmol/kg, 24.1% at 150 mmol/kg, and 16.1% at 200 mmol/kg. Results were similar when only a single measurement from each patient was used for analysis.
Limitations: Total of 29% of patients did not have concurrent spot urine osmolality and 24-hour urine osmolality. The study was conducted at a single center. Limited number of patients were on tolvaptan.
Conclusions: In adults with ADPKD, important differences exist between the 24-hour urine osmolality and spot urine osmolality that preclude interchangeable use. The method employed may impact clinical decision-making. More research is needed to determine, which urine osm should be used when assessing AVP suppression.
Keywords: Urine osmolarity; autosomal dominant polycystic kidney disease; spot and 24-hour measurement.
Plain language summary
Urine osmolality measures are used clinically to dose tolvaptan in patients with adult polycystic kidney disease. We compared urine osmolality from 24-hour and spot urine samples. We found out that important differences exist between 24-hour and spot urine samples’ osmolality. The method employed to determine urine osmolality may impact clinical decision-making in the management of patients with adult polycystic kidney disease.
© 2025 The Authors.
Figures





References
LinkOut - more resources
Full Text Sources
Miscellaneous
