

Phoenix Sepsis Criteria in Critically Ill Children: Retrospective Validation Using a United States Nine-Center Dataset, 2012-2018
- PMID: 39982153
- PMCID: PMC11792981
- DOI: 10.1097/PCC.0000000000003675
Phoenix Sepsis Criteria in Critically Ill Children: Retrospective Validation Using a United States Nine-Center Dataset, 2012-2018
Abstract
Objectives: To perform: 1) external validation of the Phoenix Sepsis Score and Phoenix sepsis criteria in a multicenter cohort of critically ill children with infection and a comparison with the 2005 International Pediatric Sepsis Consensus Conference (IPSCC) criteria; 2) a study of Phoenix sepsis criteria performance in patient subgroups based on age and comorbidities; 3) an assessment of microbiological profile of children with Phoenix sepsis; and 4) a study of the performance of the Phoenix-8 score.
Design: Secondary, retrospective analysis of a multicenter cohort study from 2012 to 2018.
Setting: Nine PICUs in the United States.
Patients: PICU admissions with suspected infection.
Interventions: None.
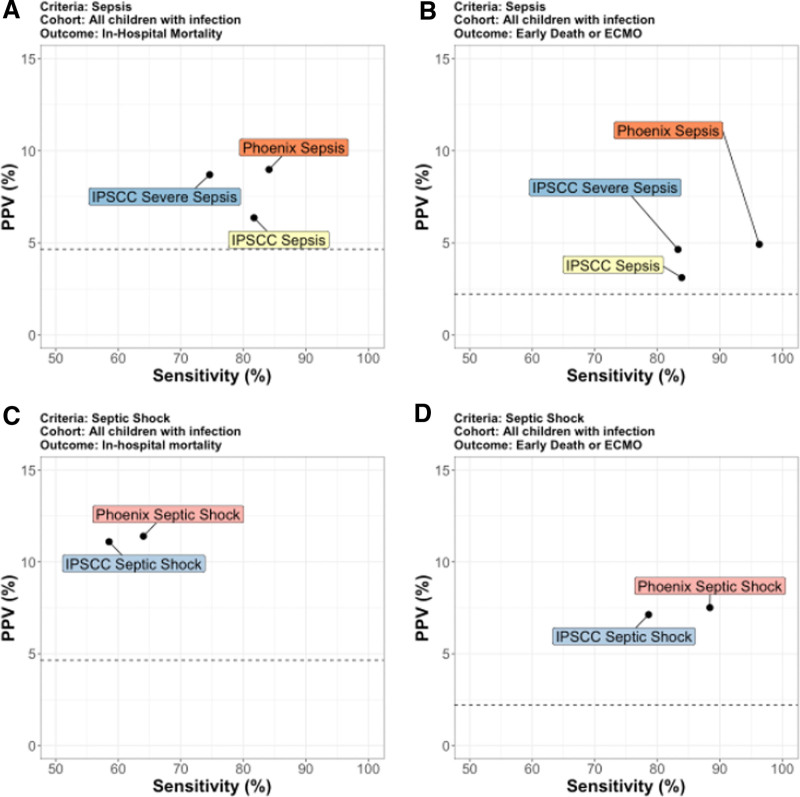
Measurements and main results: Among 25,680 encounters of children with suspected or confirmed infection on PICU admission (4.6% in-hospital mortality), 11,168 (43%) met Phoenix criteria for sepsis or septic shock (9% in-hospital mortality). The Phoenix criteria generally outperformed the IPSCC criteria at discriminating mortality in all critically ill children with infections and across all subgroup analyses, including age group, malignancy, or technology dependence. Of 11,168 patients who met Phoenix criteria, 28% were negative for IPSCC criteria for sepsis and these had higher in-hospital mortality than those who met IPSCC sepsis criteria but not Phoenix criteria (4.7% vs.1.7%; p < 0.001), which was similar to the mortality of patients without sepsis (1.3%). Sepsis was associated with respiratory or bloodstream infection, most commonly Pseudomonas aeruginosa or Staphylococcus aureus. The Phoenix-8 score had good discrimination of mortality in children with infections, comparable to or better than validated and widely used severity of illness and organ dysfunction scores.
Conclusions: In 2012-2018, among U.S. patients with suspected or confirmed infection admitted to nine PICUs, those with the highest risk of mortality can be identified using the Phoenix sepsis criteria, including in children of different age groups and those with major comorbidities.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Sanchez-Pinto’s institution received funding from the National Institute of Child Health and Human Development (NICHD; R01 HD105939); he disclosed that they own stock in llyx, Saccharo, InnoSign, and Celldom. Drs. Sanchez-Pinto, Faustino, Shah, and Bennett received support for article research from the National Institutes of Health (NIH). Dr. Atreya’s institution received funding from the National Institute of General Medical Sciences. Drs. Faustino’s and Weiss’s institutions received funding from the NIH. Dr. Khemani received funding from Orange Med/Nihon Kohden and Bayer Pharmaceuticals. Dr. Weiss’ institution received funding from the Centers for Disease Control and Prevention (CDC). Dr. Bennett’s institution received funding from the NICHD, the National Heart, Lung, and Blood Institute, the National Center for Advancing Translational Sciences, and the CDC. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

References
-
- Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric Sepsis: International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005; 6:2–8 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
