

Self-Collected Vaginal Specimens for HPV Testing: Recommendations From the Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee
- PMID: 39982254
- PMCID: PMC11939108
- DOI: 10.1097/LGT.0000000000000885
Self-Collected Vaginal Specimens for HPV Testing: Recommendations From the Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee
Abstract
Objective: The Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee developed recommendations for the use of self-collected vaginal specimens for human papillomavirus (HPV) testing in health care settings.
Methods: A comprehensive literature search was performed, external systematic reviews were evaluated, and HPV genotype agreement between self-collected vaginal and clinician-collected cervical specimens was summarized. Recommendations considered available data, public comments, and expert consensus. Recommendations were ratified through a vote by the Consensus Stakeholder Group.
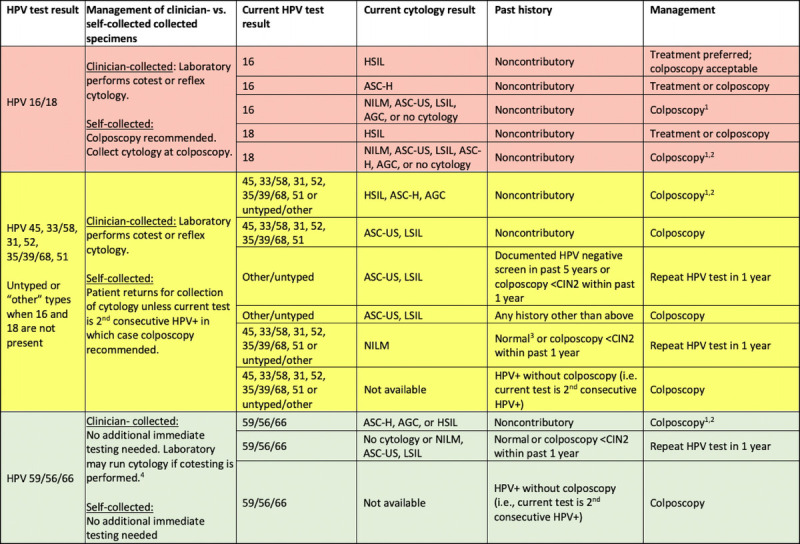
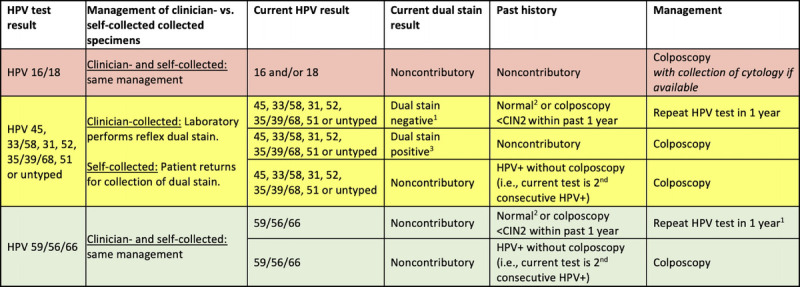
Results: Clinician-collected cervical specimens are preferred and self-collected vaginal specimens are acceptable for primary HPV screening of asymptomatic average-risk individuals. Repeat testing in 3 years is recommended following HPV-negative screens using self-collected vaginal specimens. Colposcopy with collection of cytology and biopsies is recommended following positive tests for HPV types 16 and 18. Clinician-collected cytology or dual stain for triage testing is recommended following positive tests for HPV 45, 33/58, 31, 52, 35/39/68, or 51 or for pooled HPV other types but negative for HPV 16 or 18. Repeat HPV testing in 1 year is recommended following a positive test for HPV types 56/59/66 and no other carcinogenic types. Minimal data exist on use of self-collected vaginal specimens for surveillance following abnormal screening test results, colposcopy or treatment, and therefore, clinician-collected cervical specimens are preferred.
Conclusions: Human papillomavirus testing of self-collected vaginal specimens expands cervical cancer screening options and has potential to increase access for currently underscreened individuals. Laboratory and clinical workflows will need to be modified to ensure adequate specimen processing and follow-up.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the ASCCP.
Conflict of interest statement
L.S.M. participated in an HPV vaccine call with Merck. N.B. has served on an advisory board for Merck. D.C. is a member of the United States Preventive Services Task Force (USPSTF); this article does not necessarily represent the views and policies of the USPSTF. D.C. has recused himself from development of recommendations related to screening and fully participated in recommendations related to diagnosis and management. R.S. leads guideline development at the American Cancer Society, but decisions about ACS cancer screening guidelines are made by an independent ACS Guideline Development Group; thus, this article does not necessarily represent the views of the American Cancer Society related to screening. R.S. has recused himself from the development of recommendations related to screening, but fully participated in recommendations related to diagnosis and management. M.E. has served as a consultant for Papivax, Merck, BD, PDS. R.G. has served as a consultant for Inovio. W.H. has served as a consultant for Roche, SeeGene, and AstraZeneca. R.N. has participated in an educational meeting supported by Roche. M.C. reports legal work for Merck. The other authors have declared they have no conflicts of interest.
Figures
References
-
- IARC . Cervical Cancer Screening IARC Handbooks of Cancer Prevention Volume 18. Published online 2022. Available at: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Handbooks-Of-Ca...
-
- Perkins RB Wentzensen N Guido RS, et al. . Cervical cancer screening: a review. JAMA 2023;330:547–58. - PubMed
-
- World Health Organization . WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention, second edition. Published online 2021. - PubMed
-
- Fontham ETH Wolf AMD Church TR, et al. . Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin 2020;70:321–46. - PubMed
-
- Arbyn M Castle PE Schiffman M, et al. . Meta-analysis of agreement/concordance statistics in studies comparing self- vs clinician-collected samples for HPV testing in cervical cancer screening. Int J Cancer 2022;151:308–12. - PubMed
