

Cell Lineage-Specific Differences in Clinical Behavior of Non-Functioning Pituitary Adenomas
- PMID: 39982832
- PMCID: PMC12187513
- DOI: 10.1210/clinem/dgaf112
Cell Lineage-Specific Differences in Clinical Behavior of Non-Functioning Pituitary Adenomas
Abstract
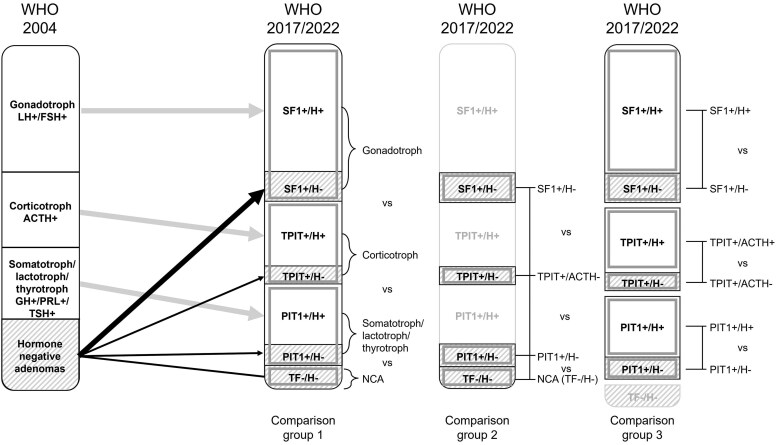
Context: Immunohistochemistry (IHC) of cell lineage-specific transcription factors (TFs) has been added to the histopathological classification of pituitary adenomas since 2017, resulting in new histopathological subtypes of TF+/hormone-non-functioning pituitary adenomas (NFPAs) and a reduction in the prevalence of null cell adenomas (NCAs).
Objective: This work aimed to evaluate associations between expression of cell lineage-specific TFs by IHC and radiological invasion and prognosis of NFPAs.
Data sources: A literature search in Medline, Embase, and CENTRAL was performed from inception up to July 11, 2023.
Study selection: Eligible studies were cohort studies reporting on radiological invasion, recurrence, and/or radiotherapy in patients with NFPAs who tested positive for one cell lineage-specific TF or negative for all 3. Finally, 27 out of 1985 studies were included.
Data extraction: Two authors independently extracted data and critically appraised risk of bias using the Quality In Prognostic Studies (QUIPS) tool.
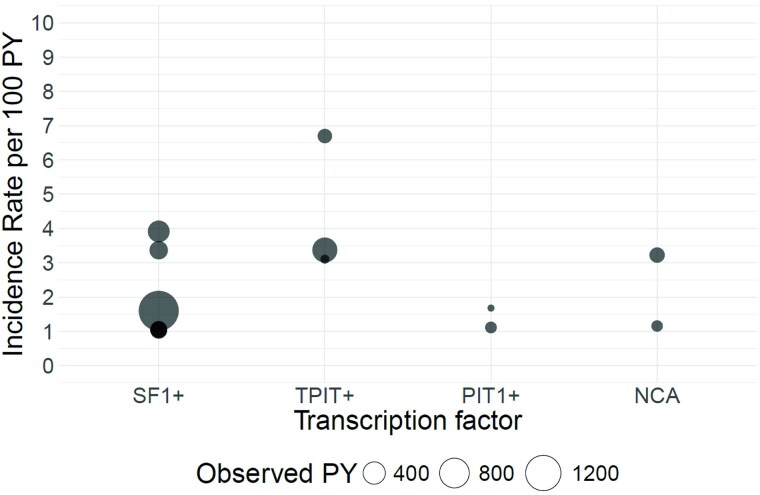
Data synthesis: Random-effects inverse variance models were used to pool effect sizes. Prevalence rate ratios (PRRs) were calculated using the Mantel-Haenszel method. Cavernous sinus invasion was more prevalent in NCAs and TPIT+ NFPAs compared with SF1+ NFPAs (PRR 1.60; 95% CI, 1.22-2.08, I2 10%, 95% prediction interval [PrI] 1.23-2.06; P = .0036, and PRR 1.43; 95% CI, 1.21-1.70, I2 0%, 95% PrI 1.17-1.76; P = .0017, respectively), and in NCAs compared with PIT1+ (PRR 1.44; 95% CI, 1.01-2.06, I2 0%, 95% PrI 0.83-2.50; P = .0454). A limited number of studies precluded data syntheses of recurrence and radiotherapy.
Conclusion: The use of cell lineage-specific TFs by IHC enables to detect histopathological subtypes of NFPAs with distinct clinical behavior.
Keywords: PitNET; SF1; TPIT; null cell adenoma; pituitary adenoma; transcription factors.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures



References
-
- Figarella-Branger D, Trouillas J. The new WHO classification of human pituitary tumors: comments. Acta Neuropathol. 2006;111(1):71‐72. - PubMed
-
- Mete O, Lopes MB. Overview of the 2017 WHO classification of pituitary tumors. Endocr Pathol. 2017;28(3):228‐243. - PubMed
-
- Asa SL, Mete O, Perry A, Osamura RY. Overview of the 2022 WHO classification of pituitary tumors. Endocr Pathol. 2022;33(1):6‐26. - PubMed
-
- Nishioka H, Inoshita N, Mete O, et al. The complementary role of transcription factors in the accurate diagnosis of clinically nonfunctioning pituitary adenomas. Endocr Pathol. 2015;26(4):349‐355. - PubMed
-
- Lenders NF, Wilkinson AC, Wong SJ, et al. Transcription factor immunohistochemistry in the diagnosis of pituitary tumours. Eur J Endocrinol. 2021;184(6):891‐901. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
