

Proprioceptive synaptic dysfunction is a key feature in mice and humans with spinal muscular atrophy
- PMID: 39982868
- PMCID: PMC12416786
- DOI: 10.1093/brain/awaf074
Proprioceptive synaptic dysfunction is a key feature in mice and humans with spinal muscular atrophy
Abstract
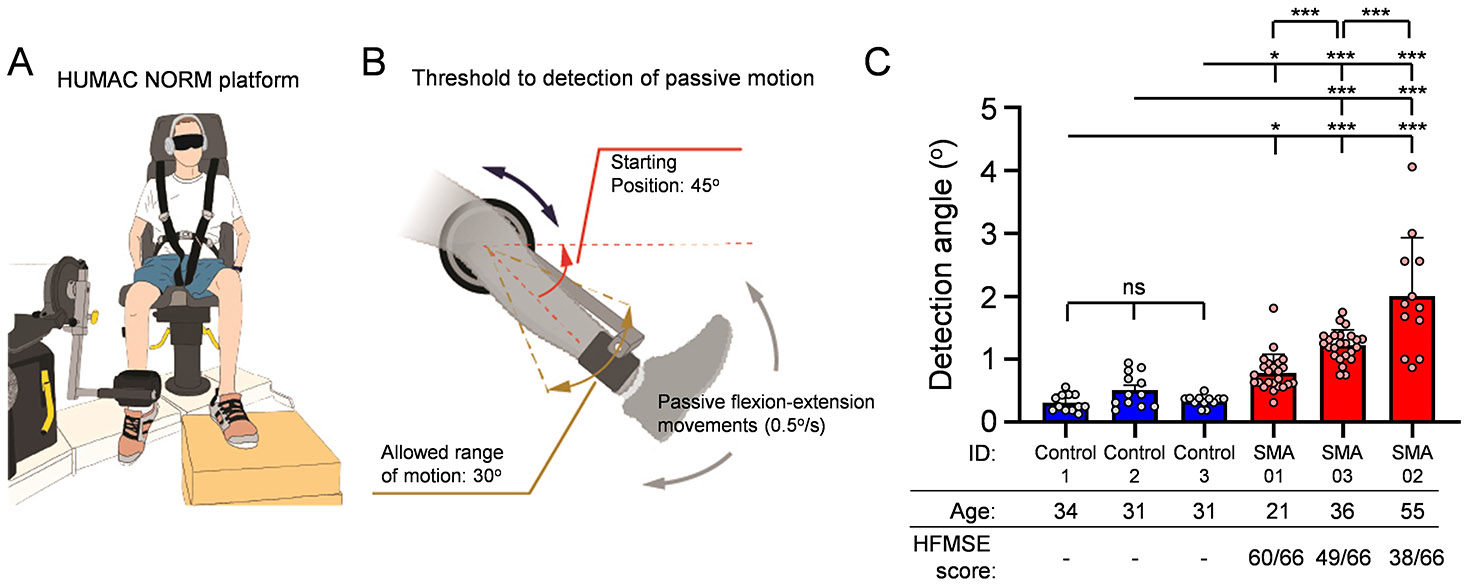
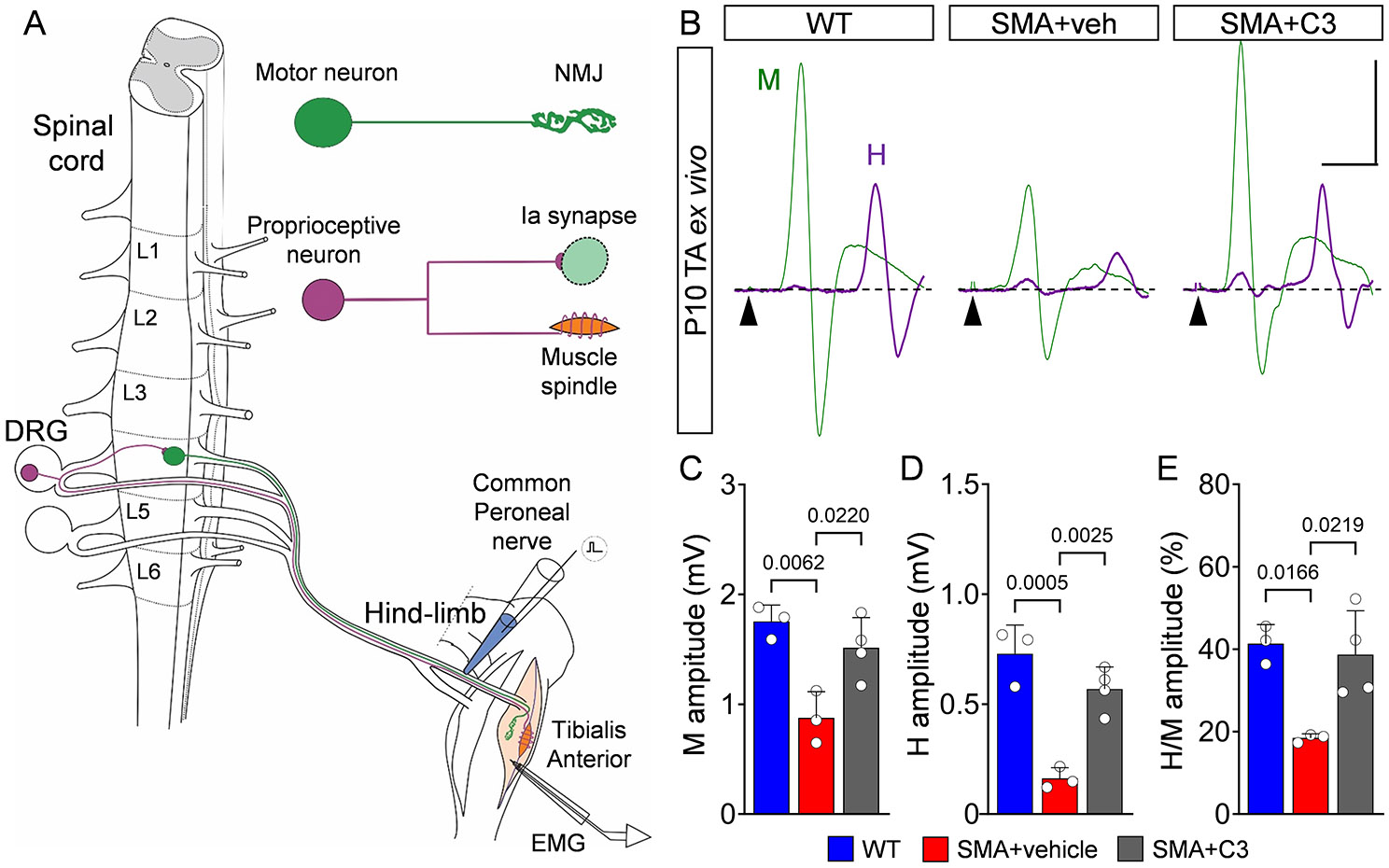
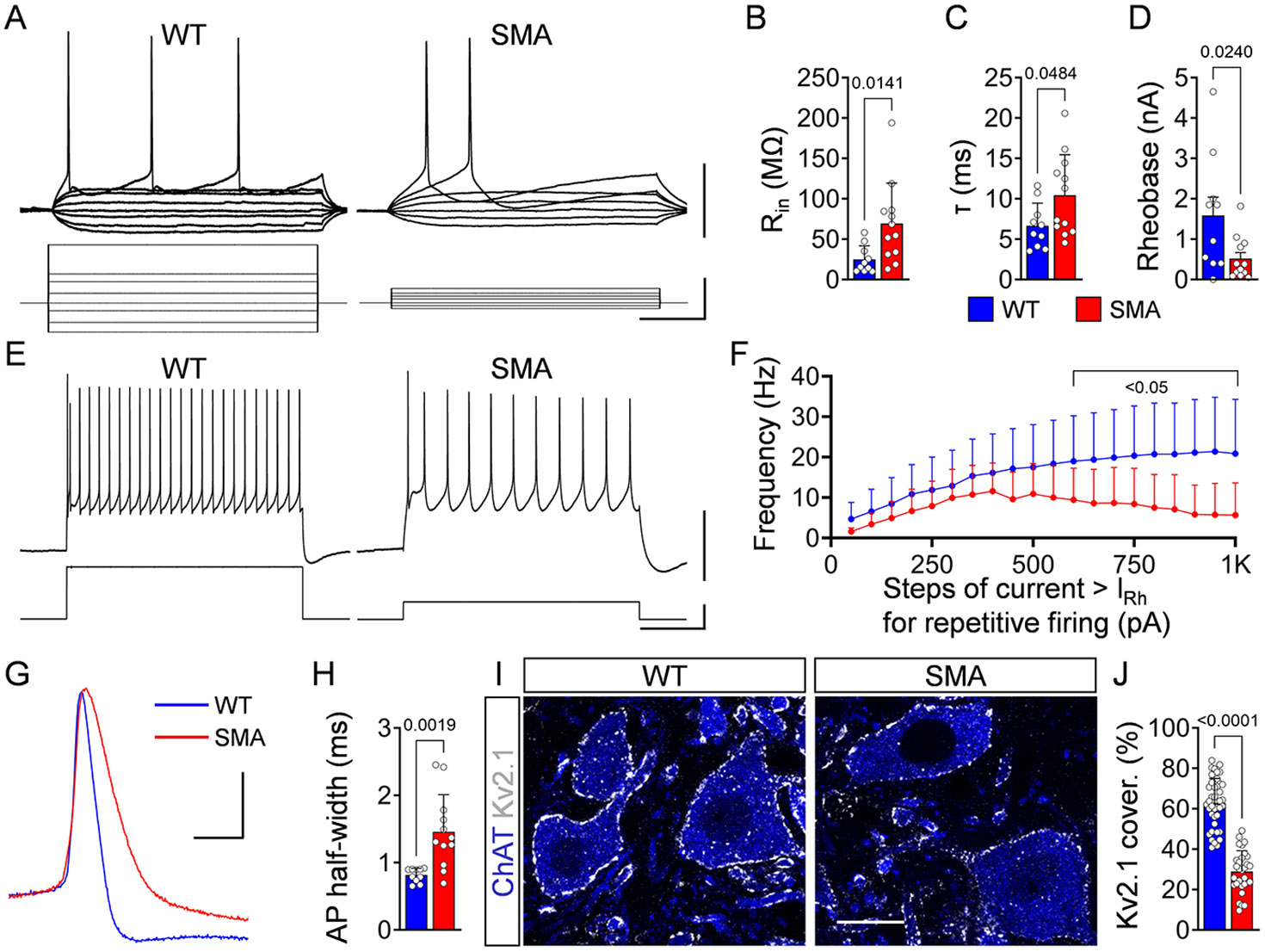
Spinal muscular atrophy (SMA) is a neurodegenerative disease characterized by a varying degree of severity that is correlated with the reduction of SMN protein levels. Motor neuron degeneration and skeletal muscle atrophy are hallmarks of SMA, but it is unknown whether other mechanisms contribute to the spectrum of clinical phenotypes. Here, through a combination of physiological and morphological studies in mouse models and SMA patients, we identify dysfunction and loss of proprioceptive sensory synapses as key signatures of SMA pathology. We demonstrate that type 3 SMA patients exhibit impaired proprioception and that their proprioceptive synapses are dysfunctional as measured by the neurophysiological test of the Hoffmann reflex. We also show moderate loss of spinal motor neurons along with reduced excitatory afferent synapses and altered potassium channel expression in motor neurons from type 1 SMA patients. These are conserved pathogenic events found in both severely affected patients and mouse models. Lastly, we report that improved motor function and fatigability in ambulatory type 3 SMA patients and mouse models treated with SMN-inducing drugs are correlated with increased function of sensory-motor circuits that can be captured accurately by the Hoffmann reflex assay. Thus, sensory synaptic dysfunction is a clinically relevant event in SMA, and the Hoffmann reflex is a suitable assay to monitor disease progression and treatment efficacy of motor circuit pathology.
Keywords: motor neuron; neurodegenerative disease; proprioception; sensory synapses; sensory–motor circuit; spinal muscular atrophy.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Figures




Update of
-
Dysfunction of proprioceptive sensory synapses is a pathogenic event and therapeutic target in mice and humans with spinal muscular atrophy.medRxiv [Preprint]. 2024 Jun 4:2024.06.03.24308132. doi: 10.1101/2024.06.03.24308132. medRxiv. 2024. Update in: Brain. 2025 Aug 1;148(8):2797-2811. doi: 10.1093/brain/awaf074. PMID: 38883729 Free PMC article. Updated. Preprint.
References
-
- Mercuri E., et al. , Spinal muscular atrophy. Nat Rev Dis Primers, 2022. 8(1): p. 52. - PubMed
MeSH terms
Grants and funding
- R35 NS122306/NS/NINDS NIH HHS/United States
- CU18-2886/Cure SMA
- Project ALS
- R01 NS116400/NS/NINDS NIH HHS/United States
- SI-1969/3-1/German Research Foundation
- R01 AA027079/AA/NIAAA NIH HHS/United States
- R01 NS125362/NS/NINDS NIH HHS/United States
- SI-1969/2-1/German Research Foundation
- R01-NS102451/ROCHE
- American SIDS Institute
- K12 HD001399/HD/NICHD NIH HHS/United States
- K01 HD084690/HD/NICHD NIH HHS/United States
- R01 NS078375/NS/NINDS NIH HHS/United States
- R01-NS114218/ROCHE
- R01 NS102451/NS/NINDS NIH HHS/United States
- K12HD001399/SMA Foundation
- K01-HD084690/Raynor Cerebellum Project
- R01-NS116400/ROCHE
- R01 NS114218/NS/NINDS NIH HHS/United States
- Grant from F. Hoffmann-La Roche
LinkOut - more resources
Full Text Sources
Medical
