

Outcomes of the COVID-19 pandemic in chronic lymphocytic leukemia: focus on the very early period and Omicron era
- PMID: 39983071
- PMCID: PMC12242415
- DOI: 10.1182/bloodadvances.2024015260
Outcomes of the COVID-19 pandemic in chronic lymphocytic leukemia: focus on the very early period and Omicron era
Abstract
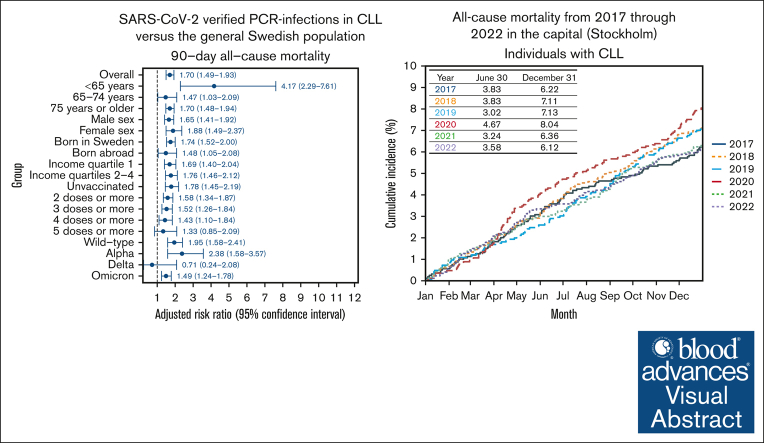
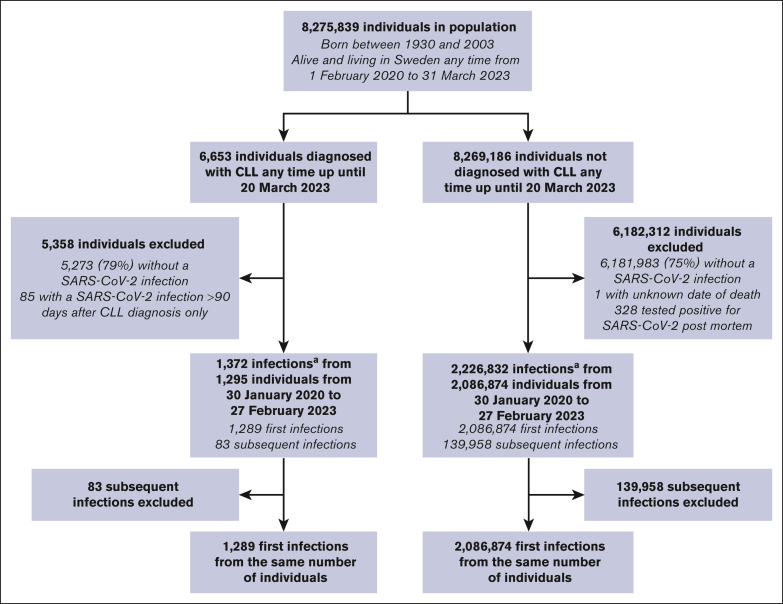
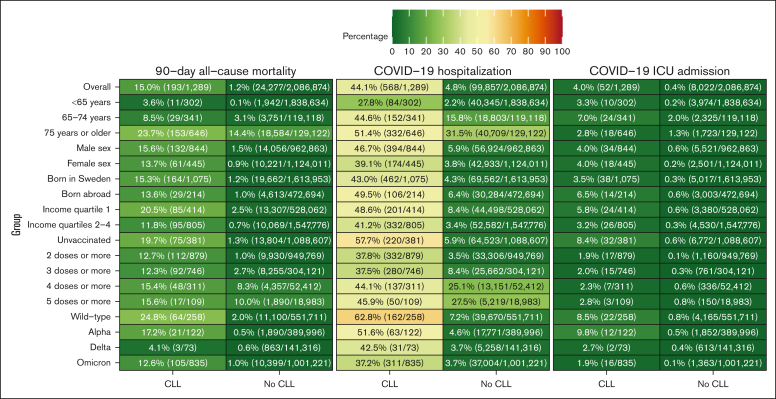
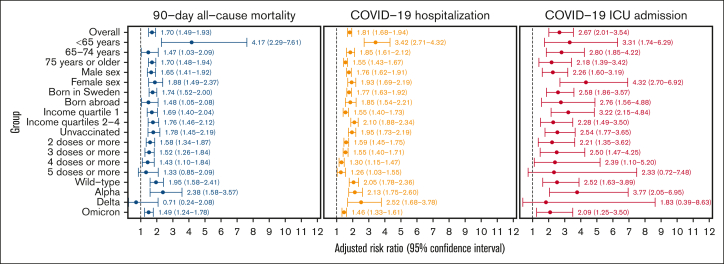
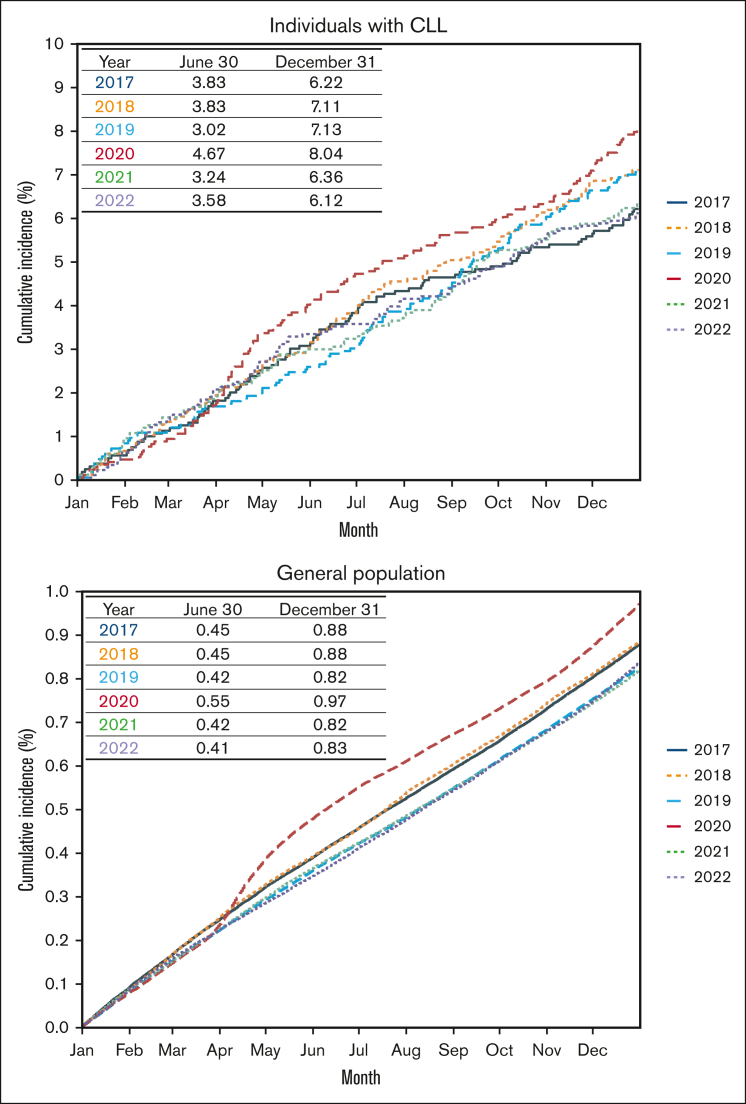
Individuals with chronic lymphocytic leukemia (CLL) face an increased risk for severe COVID-19. This study from Sweden, a country that only had a few mandatory restrictions at the onset of the pandemic, used 10 nationwide registers to compare the risks for severe COVID-19 outcomes of polymerase chain reaction-verified severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections through February 2023 in individuals with and those without CLL. From a population of 8 275 839 (6653 CLL) individuals born between 1930 and 2003, 2 088 163 first infections (1289 CLL) were included. The 90-day all-cause mortality rate and adjusted relative risk (aRR; 95% confidence interval) for individuals with CLL vs the general population was 24.8% (1.95; 1.58-2.41) during wild-type, 17.2% (2.38; 1.58-3.57) during Alpha, 4.1% (0.71; 0.24-2.08) during Delta, and 12.6% (1.49; 1.24-1.78) during Omicron infections. Their mortality during Omicron was 0.6% (<65 years), 5.4% (65-74 years), and 19.7% (≥75 years). Small molecule inhibitors (1.56; 1.03-2.37) and corticosteroid usage (1.45; 1.04-2.02) was associated with increased mortality. Next, we analyzed the all-cause mortality in the capital (Stockholm), widely affected by SARS-CoV-2 at the onset of the pandemic. Mortality in individuals with CLL increased by 55% during the first 6 months of 2020 vs 2019, and the age- and sex-aRR by 30 June was 1.53 (1.09-2.15) for individuals with CLL (P = .02) and 1.29 (1.25-1.33) for the general population (P < .001). Collectively, a significantly increased risk for severe COVID-19 and death was observed among individuals with CLL in Sweden, particularly at the onset of the pandemic when few national protective measures were introduced and also after Omicron emerged, emphasizing the need for a more pro-active pandemic strategy for CLL.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: F.K. reports funding grants from CSL Behring. P.B. reports receiving speaking and lecture fees from CSL Behring and Takeda. C.C. reports funding grants from Gilead Sciences Inc; serving as a consultant or in an advisory role for Gilead Sciences Inc and ViiV Healthcare; and speaking and lecture fees from Gilead Sciences Inc and ViiV Healthcare. S.A. reports funding grants from AbbVie and Gilead Sciences Inc, and speaking and lecture fees from AbbVie, Biogen Inc, Gilead Sciences Inc, and Merck Sharp & Dohme. A.Ö. reports funding grants from BeiGene Ltd, Lilly/Loxo Inc, and Merck Sharp & Dohme. L.H. reports funding grants from IQVIA. The remaining authors declare no competing financial interests.
Figures
Comment in
-
COVID-19 and CLL in Sweden: lessons learned?Blood Adv. 2025 Jul 8;9(13):3223-3225. doi: 10.1182/bloodadvances.2025016266. Blood Adv. 2025. PMID: 40569632 Free PMC article. No abstract available.
References
-
- Hamblin AD, Hamblin TJ. The immunodeficiency of chronic lymphocytic leukaemia. Br Med Bull. 2008;87:49–62. - PubMed
-
- Mauro FR, Giannarelli D, Galluzzo CM, et al. Response to the conjugate pneumococcal vaccine (PCV13) in patients with chronic lymphocytic leukemia (CLL) Leukemia. 2021;35(3):737–746. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
