

Optimizing spatial normalization of multisubject inner ear MRI: comparison of different geometry-preserving co-registration approaches
- PMID: 39984604
- PMCID: PMC11845522
- DOI: 10.1038/s41598-025-90842-2
Optimizing spatial normalization of multisubject inner ear MRI: comparison of different geometry-preserving co-registration approaches
Abstract
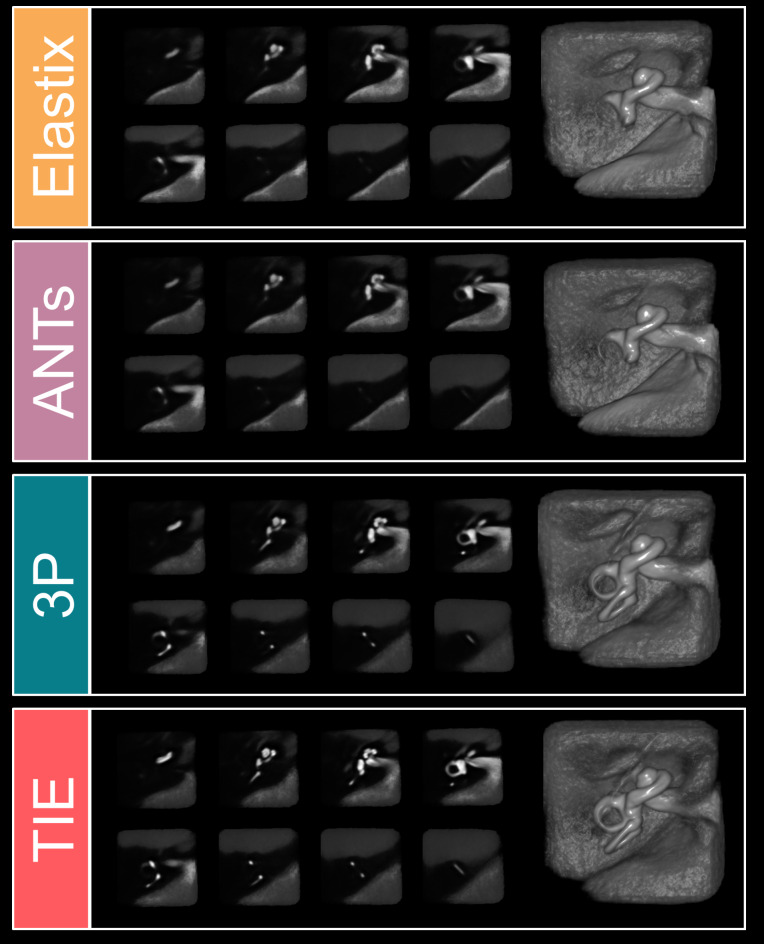
Spatial normalization of multisubject inner ear imaging data is challenging, due to both substantial intraindividual differences and the small size of the organ compared to other intracranial structures. Automatic whole brain co-registration to standard space can only roughly co-align the peripheral vestibular endorgan, and complemental manual registration is highly time-consuming. Here, we compared the accuracy of four geometry-maintaining co-registration methods (one semi-manual method and three automatic methods). High-resolution structural T2-MRI of 153 inner ears from patients and healthy participants were co-registered to an inner-ear atlas. The semi-manual method used a three-point landmark-based approach (3P), two automatic methods were based on unassisted standard algorithms (Advanced Normalization Tools (ANTs), Elastix (EL)), while the fourth automatic method utilized a volumetrically dilated, atlas-based mask (thick inner ear, TIE) for probabilistic inner ear masking. Registration accuracy was evaluated by neurotologists blinded to the respective registration paradigm, and the resulting median volumes were quantified using colocalization analyses. The mask-aided automatic approach showed the best ratings, followed by the semi-manual three-point landmark-based registration (mean ratings (lower: better) TIE 2.21 ± 1.15; 3P 2.58 ± 0.61; EL 3.42 ± 1.06; ANTs 3.49 ± 1.26). The semi-manual method had the lowest rate of insufficient registrations, followed by TIE (3P: 3.70%; TIE: 8.28%; EL: 22.66%; ANTs: 27.02%). TIE showed the highest colocalization metrics with the atlas. Only TIE and 3P allowed for sufficient semicircular canal visualization in method-wise average volumes. Overall, geometry-preserving spatial normalization of multisubject inner ear imaging data is possible and could allow groupwise examinations of the bony labyrinth or temporal bone morphology in the future.
Keywords: Atlas; Endolymphatic hydrops; Inner ear; Peripheral vestibular system; Spatial normalization; Vertigo.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
A probabilistic atlas of the human inner ear's bony labyrinth enables reliable atlas-based segmentation of the total fluid space.J Neurol. 2019 Sep;266(Suppl 1):52-61. doi: 10.1007/s00415-019-09488-6. Epub 2019 Aug 17. J Neurol. 2019. PMID: 31422454
-
Validation of inner ear MRI in patients with Ménière's disease by comparing endolymphatic hydrops from histopathologic specimens.Sci Rep. 2021 Sep 6;11(1):17738. doi: 10.1038/s41598-021-97213-7. Sci Rep. 2021. PMID: 34489538 Free PMC article.
-
Automatic measurement of the labyrinth using image registration and a deformable inner ear atlas.Acad Radiol. 2003 Sep;10(9):988-99. doi: 10.1016/s1076-6332(03)00121-1. Acad Radiol. 2003. PMID: 13678087
-
Some Remarks on Imaging of the Inner Ear: Options and Limitations.Clin Neuroradiol. 2015 Oct;25 Suppl 2:197-203. doi: 10.1007/s00062-015-0422-y. Epub 2015 Jul 8. Clin Neuroradiol. 2015. PMID: 26153464 Review.
-
Brain and inner-ear fluid homeostasis, cochleovestibular-type tinnitus, and secondary endolymphatic hydrops.Int Tinnitus J. 2006;12(1):75-81. Int Tinnitus J. 2006. PMID: 17147045 Review.
Cited by
-
Contrast Agent Uptake in Endolymphatic Sac and Duct: Inverse Relation to Endolymphatic Hydrops.Laryngoscope. 2025 Aug;135(8):2914-2922. doi: 10.1002/lary.32127. Epub 2025 Mar 19. Laryngoscope. 2025. PMID: 40105260 Free PMC article.
References
-
- Cortés-Domínguez, I., Fernández-Seara, M. A., Pérez-Fernández, N. & Burguete, J. Systematic method for morphological reconstruction of the semicircular canals using a fully automatic skeletonization process. Appl. Sci.9, 4904 (2019).
-
- Lewis, M. A. et al. The spectrum of cochlear malformations in CHARGE syndrome and insights into the role of the CHD7 gene during embryogenesis of the inner ear. Neuroradiology65, 819–834 (2023). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
