

Quantitative beam optimization for radiotherapy of peripheral lung lesions: A pilot study in stereotactic body radiotherapy
- PMID: 39985560
- PMCID: PMC11969078
- DOI: 10.1002/acm2.70029
Quantitative beam optimization for radiotherapy of peripheral lung lesions: A pilot study in stereotactic body radiotherapy
Abstract
Background: To quantify beam optimization for stereotactic body radiotherapy (SBRT) of peripheral lung lesions.
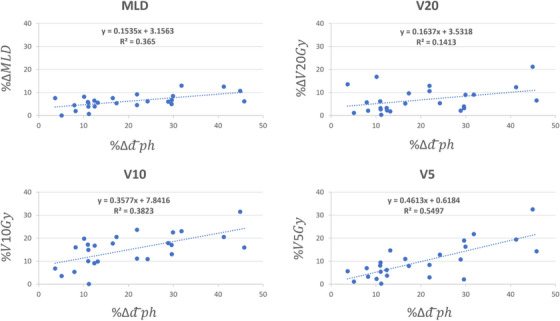
Method: The new beam optimization approach was based on maximizing the therapeutic gain (TG) of the beam set by minimizing the average physical depth of the lesion with respect to the beam's eye view (BEV). The new approach was evaluated by replanning the 25 SBRT lesions retrospectively to assess if a better plan is achievable in all aspects. Difference in 25 Gy isodose line volume (IDLV25 Gy), IDLV20 Gy, IDLV15 Gy, IDLV10 Gy, and IDLV5 Gy between the two plan cohorts were calculated as a measure of plan size and fitted in a linear regression model against the changes in the lesion depth with respect to the BEV to assess the relationship between the changes in the treatment depth and that of the plan size.
Results: Beam optimization achieved a better plan in all cases by lowering the depth of treatment with an average of % 20.03 ± 12.30 (3.66%-45.78%). As the depth of treatment decreases, the size of the plan also decreases. We observed a reduction of % 4.64 ± 4.55 (0.02%-21.58%, p < 3.8 × 10-5), %5.16 ± 5.54 (0.03%-24.68%, p < 0.005), %6.46 ± 6.95 (-1.35%-29.05%, p < 0.009), %12.83 ± 9.06 (0.89%-37.65%, p < 0.0001), and %14.01 ± 9.87 (1.43%-41.84%, p < 4.5 × 10-6) in IDLV25 Gy, IDLV20 Gy, IDLV15 Gy, IDLV10 Gy, and IDLV5 Gy, respectively.
Conclusion: Physical depth of the lesion with respect to the BEV is inversely proportional to the TG of a beam-set and can be used as a robust and standard metric to select an appropriate beam-set for SBRT of the peripheral lung lesions. Further evaluation warrants the utility of such concept in routine clinical use.
Keywords: SBRT; beam optimization; integral dose; therapeutic gain.
© 2025 The Author(s). Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






References
-
- Lung Cancer Statistics | How Common is Lung Cancer? Accessed April 26, 2024. https://www.cancer.org/cancer/types/lung‐cancer/about/key‐statistics.html
-
- Lung Cancer—Non‐Small Cell—Statistics. Cancer.Net. June 25, 2012. Accessed April 26, 2024. https://www.cancer.net/cancer‐types/lung‐cancer‐non‐small‐cell/statistics
-
- Stanic S, Paulus R, Timmerman RD, et al. No clinically significant changes in pulmonary function following stereotactic body radiation therapy for early‐ stage peripheral non‐small cell lung cancer: an analysis of RTOG 0236. Int J Radiat Oncol Biol Phys. 2014;88(5):1092‐1099. doi:10.1016/j.ijrobp.2013.12.050 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
