

Long-term clinical outcome of 103 patients with acromegaly after pituitary surgery
- PMID: 39987353
- PMCID: PMC11846723
- DOI: 10.1007/s11102-025-01503-6
Long-term clinical outcome of 103 patients with acromegaly after pituitary surgery
Abstract
Purpose: Acromegaly is a rare disease that can be challenging to treat due to residual pituitary adenoma after surgery or variable response to medical treatments. The primary aim of the study was to evaluate the path of treatment and long-term outcome of acromegaly after pituitary surgery.
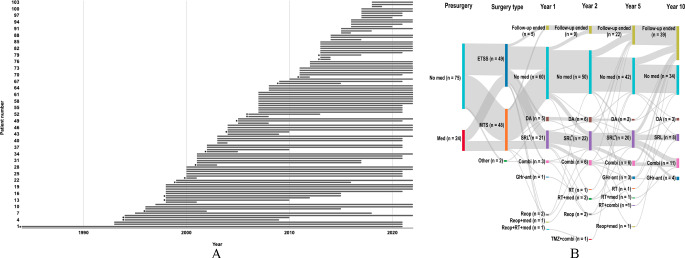
Methods: Patients with acromegaly who had undergone surgery for a growth hormone-producing pituitary neuroendocrine tumor also known as a pituitary adenoma, at Sahlgrenska University Hospital between 1994 and 2019 were included in the study. Medical records from diagnosis to the end of study (November 2022) were reviewed for surgical outcome and treatment patterns related to acromegaly.
Results: In the cohort of 103 patients, 111 surgeries were performed. Mean follow-up duration was 12.7 (range: 0-37) years. Lesions were identified as a macroadenoma in 76 (76.8%) cases. At post-surgical follow-up until discharge from hospital, surgical complications and new pituitary hormone deficiency or syndrome of inappropriate antidiuretic hormone secretion occurred in 37% of cases. At 1-year post-surgery follow-up, 50% of evaluable patients achieved biochemical control of acromegaly. Of the 96 patients who had follow-up > 1 year, 53 (51.5%) had no additional medication for acromegaly after surgery until end of their follow-up. From diagnosis to the end of follow-up, 53 patients received medical therapy and seven were treated with radiotherapy.
Conclusion: About half of the patients had biochemical control of acromegaly 1-year post-surgery. Treatment patterns reflected the complexity of post-surgical management and provided an overview of the long-term clinical progression in patients with acromegaly following pituitary surgery.
Keywords: Acromegaly; Growth hormone; Pituitary adenoma; Pituitary neuroendocrine tumor; Transsphenoidal surgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Institutional review board statement: The study was approved by the Swedish Ethical Review Authority (Etikprövningsmyndigheten) (Dnr: 2019–04779). Competing interests: A.P., T.O.B., T.S., T.H., H.C., and G.J. has no conflict of interest to declare. D.E. has received lecture fees from Ipsen, Pfizer AB and Recordati Rare Disease. D.S.O. has been a consultant for Sandoz, Ipsen, and Pfizer; has received unrestricted grants from Sandoz and Pfizer; and is an employee at AstraZeneca as of 8 August 2021.
Figures
References
-
- Crisafulli S, Luxi N, Sultana J et al (2021) Global epidemiology of acromegaly: a systematic review and meta-analysis. Eur J Endocrinol 185(2):251–263. 10.1530/EJE-21-0216 - PubMed
-
- Campbell PG, Kenning E, Andrews DW, Yadla S, Rosen M, Evans JJ (2010) Outcomes after a purely endoscopic transsphenoidal resection of growth hormone-secreting pituitary adenomas. Neurosurg Focus 29(4):E5. 10.3171/2010.7.FOCUS10153 - PubMed
-
- Buchfelder M, Schlaffer SM (2017) The surgical treatment of acromegaly. Pituitary 20(1):76–83. 10.1007/s11102-016-0765-7 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
