

Efficacy of cardiac myosin inhibitors mavacamten and aficamten in hypertrophic cardiomyopathy: a systematic review and meta-analysis of randomised controlled trials
- PMID: 39988344
- PMCID: PMC11848667
- DOI: 10.1136/openhrt-2025-003215
Efficacy of cardiac myosin inhibitors mavacamten and aficamten in hypertrophic cardiomyopathy: a systematic review and meta-analysis of randomised controlled trials
Abstract
Background: Unlike other suggested therapies, myosin inhibitors have been shown to change the course of hypertrophic cardiomyopathy by altering the contractile mechanics of cardiomyocytes. This meta-analysis sought to determine the efficacy of mavacamten and aficamten in hypertrophic cardiomyopathy.
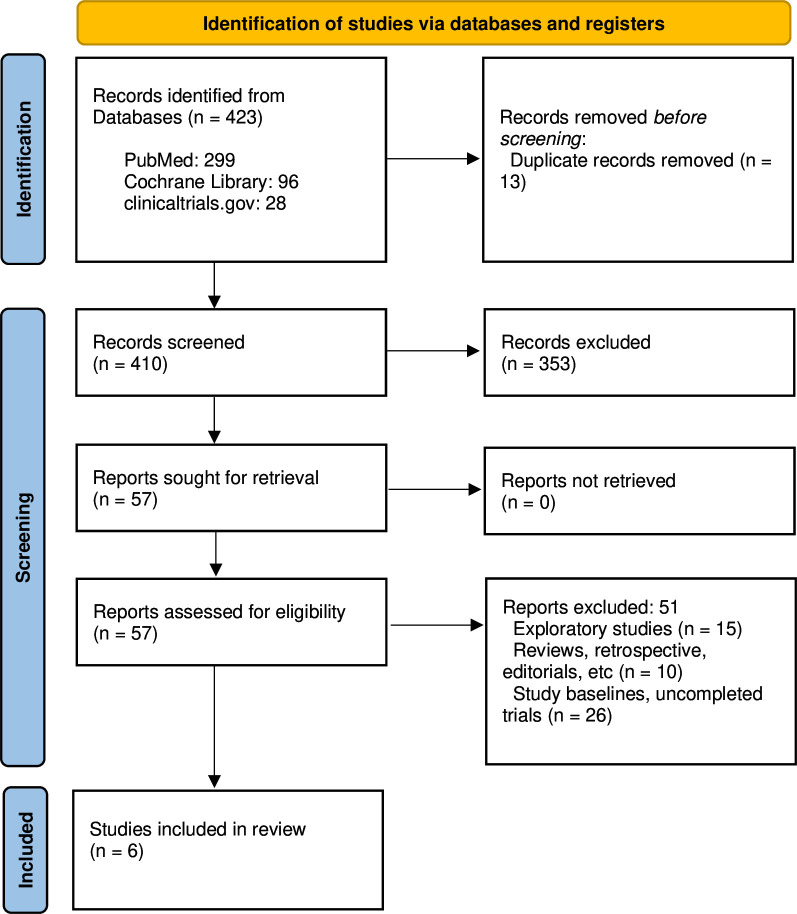
Methods: The online databases were searched from inception to July 2024, including the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, ClinicalTrials.gov. The meta-analytical data were pooled using risk ratios (RRs) with 95% CI, standard mean difference (SMD) and SE.
Results: A total of 6 randomised controlled trials with 826 hypertrophic cardiomyopathy patients (mean age±SD up to 59.8±14.2 years in intervention vs 60.9±10.5 years in placebo) were included in our study. Of these, 443 received a cardiac myosin inhibitor and 383 received a placebo. The resting left ventricular outflow tract (LVOT) gradient between the two groups was considerably improved by cardiac myosin inhibitors (MD -57.27; 95% CI -63.05 to -51.49). Significant differences were also observed in the post-Valsalva LVOT gradient between the two groups (MD -55.86; 95% CI -65.55 to -46.18). Significantly decreased left ventricle ejection fraction (LVEF) was also seen (MD -4.74; 95% CI -7.22 to -2.26). The New York Health Association (NYHA) class improvement between the two groups also changed significantly (RR 2.21; 95% CI 1.75 to 2.80). Cardiac myosin inhibitors also caused significant improvement in the Kansas City Cardiomyopathy Questionnaire in a Clinical Summary Score between the two groups (MD 7.71; 95% CI 5.37 to 10.05) and significant reduction in the N-terminal pro-B-type natriuretic peptide (SMD -13.27; 95% CI -17.51 to -9.03) and the cardiac troponin I (SMD -11.90; 95% CI -15.07 to -8.72).
Conclusion: According to our meta-analysis, cardiac myosin inhibitors significantly improve the resting and post-Valsalva LVOT gradient, reduce the LVEF and improve the NYHA class and cardiac biomarkers when compared with the placebo.
Prospero registration number: CRD52024586161.
Keywords: Cardiomyopathies; Cardiomyopathy, Hypertrophic; Meta-Analysis.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures














References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials