

A pictorial essay on cross-sectional imaging findings of pathologies in the second (D2) segment of the duodenum in adults
- PMID: 39988596
- PMCID: PMC12331787
- DOI: 10.1007/s00261-025-04846-7
A pictorial essay on cross-sectional imaging findings of pathologies in the second (D2) segment of the duodenum in adults
Abstract
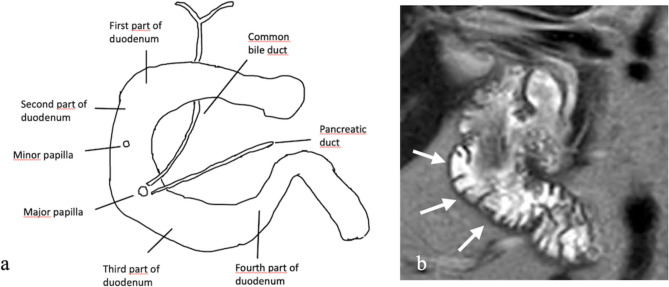
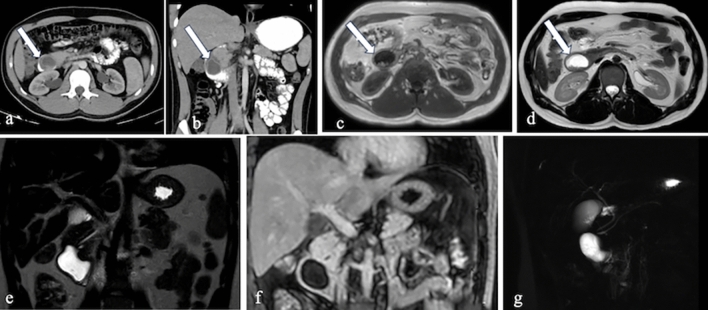
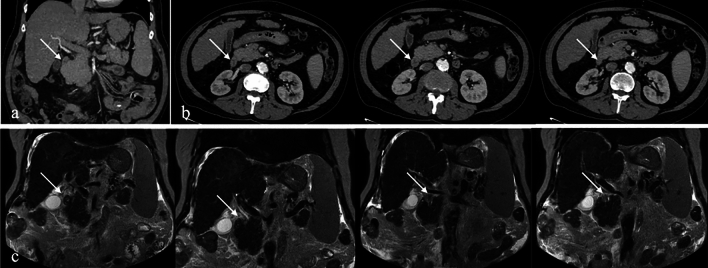
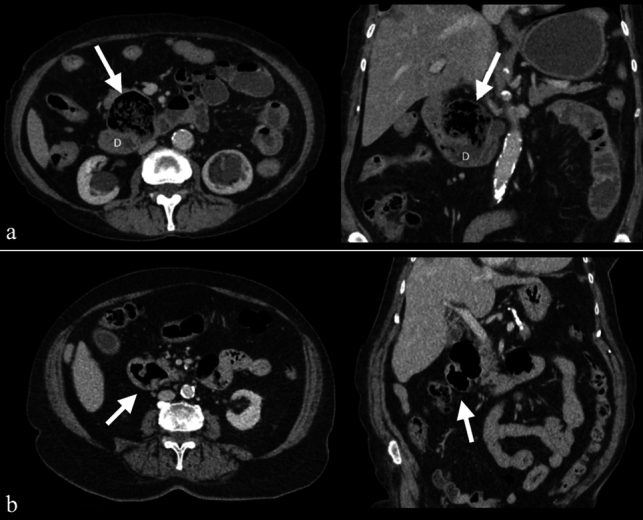
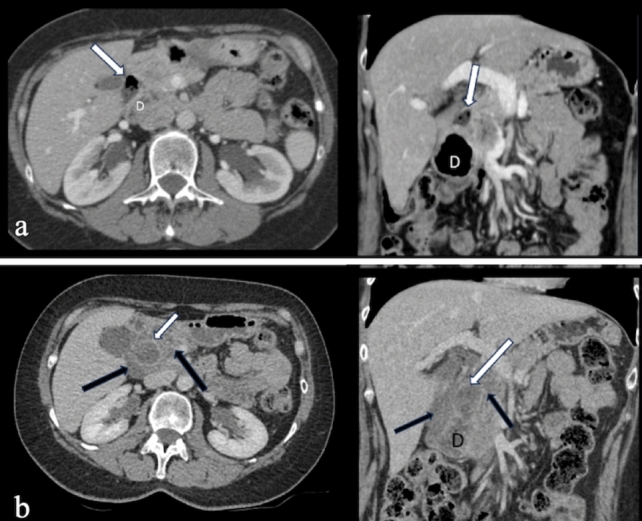
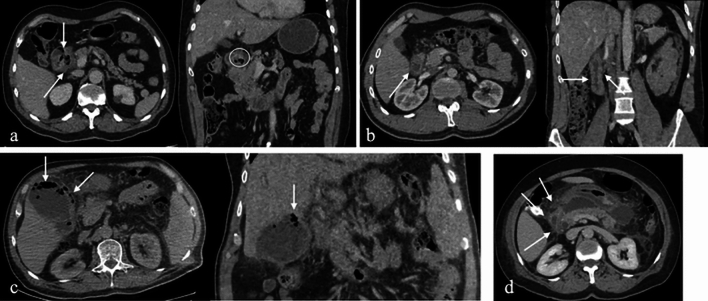
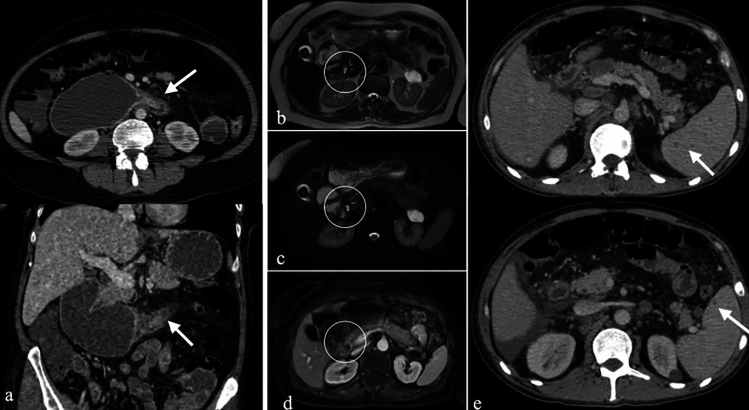
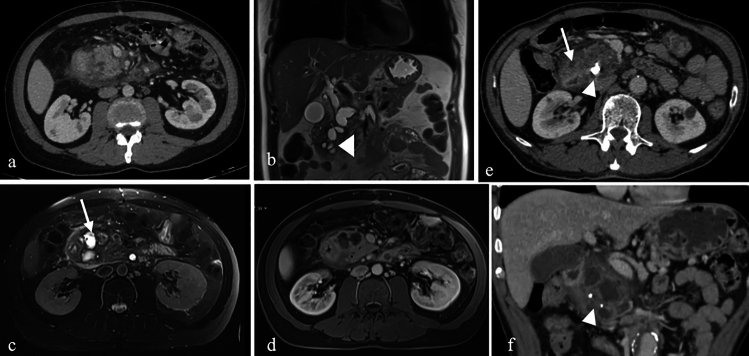
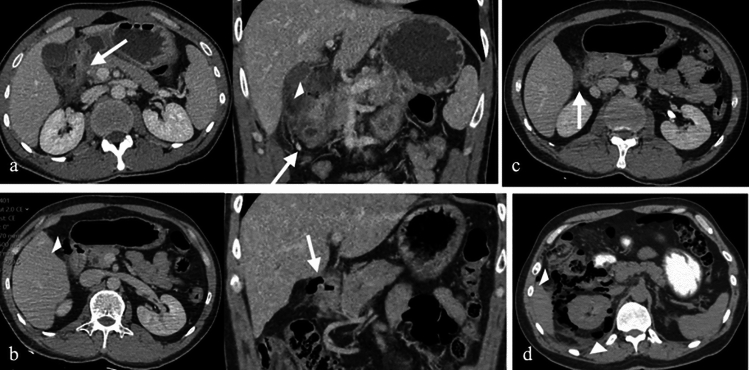
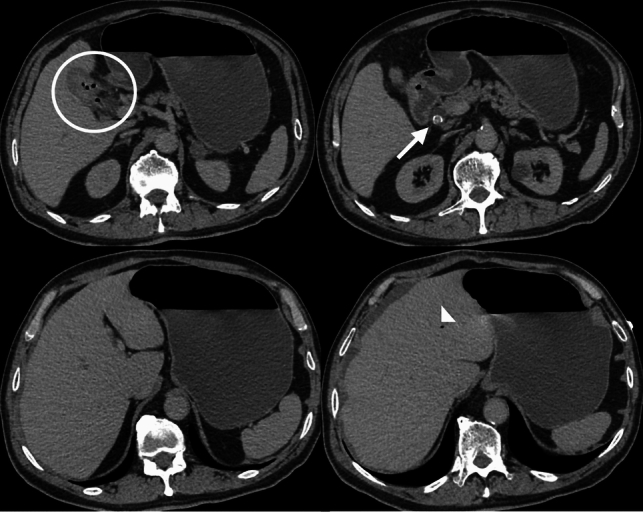
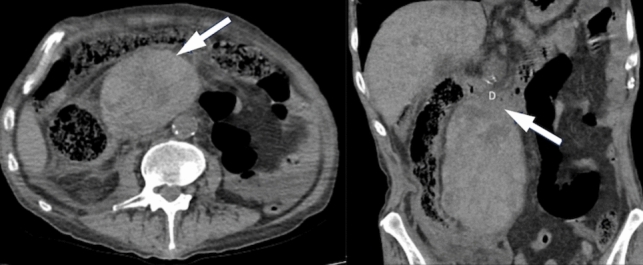
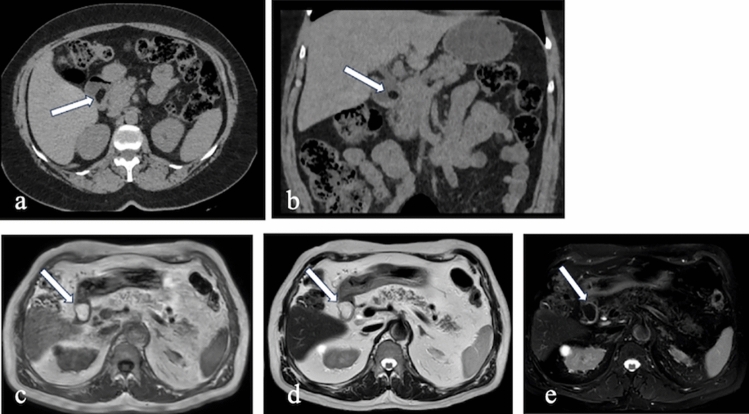
The duodenum, the initial segment of the small intestine, is divided into four parts: the superior (D1), descending (second) (D2), horizontal (D3), and ascending (D4) segments. Despite its short length, the descending part (D2 segment) holds clinical significance due to its anatomical proximity to structures such as the gallbladder, right kidney, colon, and pancreas. This anatomical localization and contiguity give rise to various pathologies, including congenital, inflammatory, infectious, neoplastic, vascular, and traumatic conditions. Cross-sectional imaging modalities play a pivotal role in evaluating pathologies of the second (D2) segment of the duodenum. This article aims to provide a comprehensive overview of these pathologies and delineate their imaging characteristics.
Keywords: Computed tomography; Duodenum; Magnetic resonance imaging; Neoplastic pathologies; Non-neoplastic pathologies.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests.
Figures

Similar articles
-
Imaging spectrum of nonneoplastic duodenal diseases.Clin Imaging. 2016 Nov-Dec;40(6):1173-1181. doi: 10.1016/j.clinimag.2016.08.007. Epub 2016 Aug 6. Clin Imaging. 2016. PMID: 27572283
-
Revolutionizing the Pancreatic Tumor Diagnosis: Emerging Trends in Imaging Technologies: A Systematic Review.Medicina (Kaunas). 2024 Apr 24;60(5):695. doi: 10.3390/medicina60050695. Medicina (Kaunas). 2024. PMID: 38792878 Free PMC article.
-
Radiofrequency ablation of liver metastases in a patient with pancreatic cancer and long-term survival: A case report.World J Clin Cases. 2025 Jul 16;13(20):100169. doi: 10.12998/wjcc.v13.i20.100169. World J Clin Cases. 2025. PMID: 40671744 Free PMC article.
-
MarkVCID cerebral small vessel consortium: II. Neuroimaging protocols.Alzheimers Dement. 2021 Apr;17(4):716-725. doi: 10.1002/alz.12216. Epub 2021 Jan 21. Alzheimers Dement. 2021. PMID: 33480157 Free PMC article.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
References
-
- Ryan S, McNicholas M, Eustace SJ (2024) Anatomy for Diagnostic Imaging. Saunders, Elsevier.
-
- Butler P, Mitchell A, Healy JC et al. (2012) Applied Radiological Anatomy Cambridge University Press.
-
- Gosangi B, Rocha TC, Duran-Mendicuti A (2020) Imaging Spectrum of Duodenal Emergencies. Radiographics 40:1441–1457. 10.1148/rg.2020200045 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
