

Health Care Use and Expenditures Associated With Cardiac Rehabilitation Among Eligible Medicare Fee-for-Service Beneficiaries
- PMID: 39989369
- PMCID: PMC12132668
- DOI: 10.1161/JAHA.124.037811
Health Care Use and Expenditures Associated With Cardiac Rehabilitation Among Eligible Medicare Fee-for-Service Beneficiaries
Abstract
Background: Cardiac rehabilitation (CR) can improve cardiovascular health. We identified whether CR participation was associated with fewer subsequent inpatient hospitalizations and emergency department visits and less Medicare and out-of-pocket expenditures, and whether outcomes varied by amount of participation.
Methods: This retrospective study used Medicare fee-for-service claims data, including beneficiaries with a CR-qualifying event in 2016. Participants attended ≥2 sessions of CR within 365 days of the event. Propensity score matching was used to identify CR-eligible nonparticipants. Difference-in-differences analyses were used to compare differences in outcomes before (2014-2015) and after (2018-2019; 2-year CR period=2016-2017) the CR period between participants and nonparticipants.
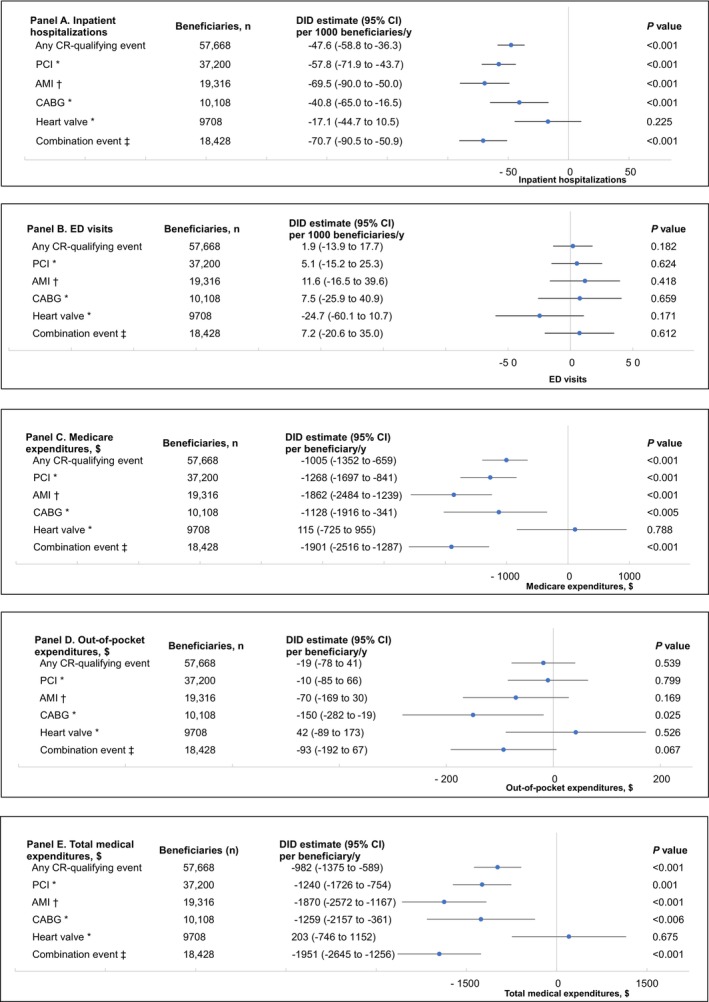
Results: We identified 57 668 CR-eligible beneficiaries after matching, with equal numbers of participants and nonparticipants. Nearly 65% of beneficiaries had a percutaneous coronary intervention, 33.5% had an acute myocardial infarction, 17.5% had a coronary artery bypass graft, and 16.8% had a heart valve repair/replacement. Compared with nonparticipants, participants had 47.6 fewer subsequent annual inpatient hospitalizations per 1000 beneficiaries (95% CI, -58.8 to -36.3) and $1005 lower subsequent annual Medicare expenditures per beneficiary (95% CI, -$1352 to -$659). Compared with no participation, medium participation (12-23 sessions), high participation (24-35 sessions), and CR completion (≥36 sessions) were associated with fewer inpatient hospitalizations and lower Medicare expenditures per year.
Conclusions: CR was associated with fewer subsequent annual inpatient hospitalizations and lower subsequent annual Medicare expenditures. A higher amount of participation was associated with a further reduction in hospitalizations and expenditures. These findings can inform programs and policies that encourage CR participation.
Keywords: cardiac rehabilitation; emergency department visits; expenditures; inpatient hospitalizations.
Conflict of interest statement
None.
Figures

Similar articles
-
Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative.Circ Cardiovasc Qual Outcomes. 2020 Jan;13(1):e005902. doi: 10.1161/CIRCOUTCOMES.119.005902. Epub 2020 Jan 14. Circ Cardiovasc Qual Outcomes. 2020. PMID: 31931615 Free PMC article.
-
Mortality, Hospitalizations, and Expenditures for the Medicare Population Aged 65 Years or Older, 1999-2013.JAMA. 2015 Jul 28;314(4):355-65. doi: 10.1001/jama.2015.8035. JAMA. 2015. PMID: 26219053 Free PMC article.
-
Association of Cardiac Rehabilitation With Decreased Hospitalization and Mortality Risk After Cardiac Valve Surgery.JAMA Cardiol. 2019 Dec 1;4(12):1250-1259. doi: 10.1001/jamacardio.2019.4032. JAMA Cardiol. 2019. PMID: 31642866 Free PMC article.
-
Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials.JAMA. 2009 Feb 11;301(6):603-18. doi: 10.1001/jama.2009.126. JAMA. 2009. PMID: 19211468 Clinical Trial.
-
Effects of liposomal bupivacaine (LB) and provider experience with LB on service utilization, clinical outcomes, and Medicare expenditures among fee-for-service (FFS) beneficiaries.J Med Econ. 2025 Dec;28(1):848-858. doi: 10.1080/13696998.2025.2510814. Epub 2025 Jun 4. J Med Econ. 2025. PMID: 40434805
References
-
- About Million Hearts® 2027 . Million Hearts®. Accessed September 7, 2022. https://millionhearts.hhs.gov/about‐million‐hearts/index.html.
-
- 42 c.F.R 410.49, cardiac rehabilitation program and intensive cardiac rehabilitation program: Conditions of coverage. Accessed April 14, 2024. https://www.ecfr.gov/current/title‐42/chapter‐IV/subchapter‐B/part‐410/s....
-
- Patel DK, Duncan MS, Shah AS, Lindman BR, Greevy RA Jr, Savage PD, Whooley MA, Matheny ME, Freiberg MS, Bachmann JM. Association of cardiac rehabilitation with decreased hospitalization and mortality risk after cardiac valve surgery. JAMA Cardiol. 2019;4:1250–1259. doi: 10.1001/jamacardio.2019.4032 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
