

Reintegration Into the Workforce After Kidney Transplantation Based on Urbanization Status in Switzerland
- PMID: 39990912
- PMCID: PMC11843122
- DOI: 10.1016/j.ekir.2024.10.029
Reintegration Into the Workforce After Kidney Transplantation Based on Urbanization Status in Switzerland
Abstract
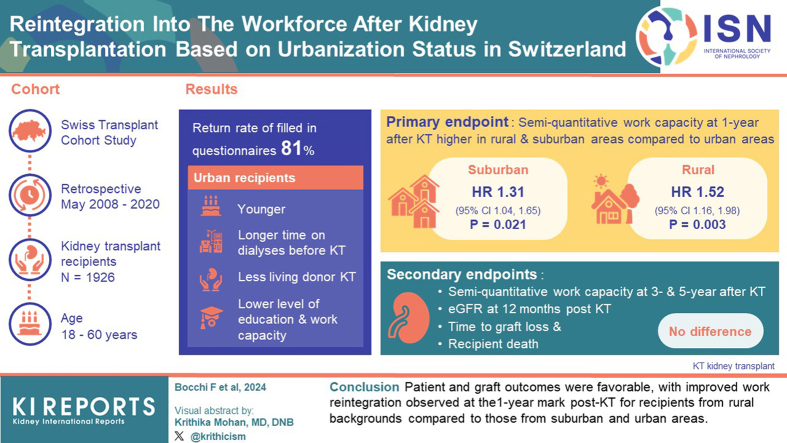
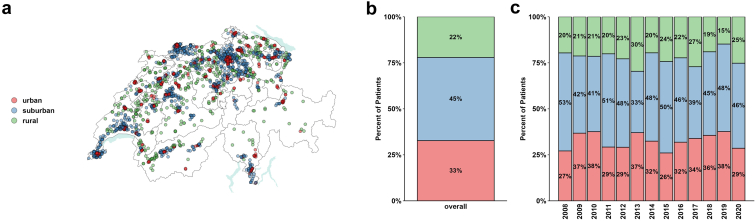
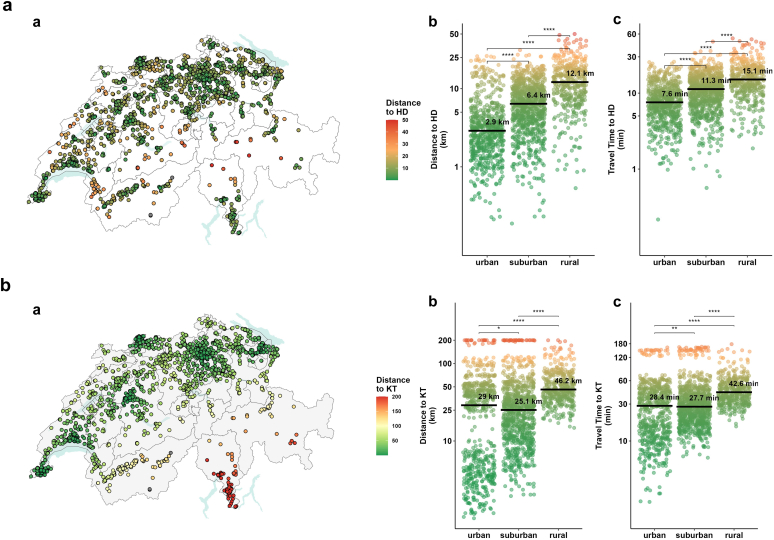
Introduction: Most of Switzerland's population and employment opportunities are concentrated in urban areas. Although kidney transplantation (KT) is the preferred therapy for eligible candidates, individuals in rural areas face challenges accessing specialized medical services due to longer travel distances. Limited understanding exists regarding patients' perspectives on returning to work after KT and whether this correlates with their urbanization status, potentially influencing outcomes.
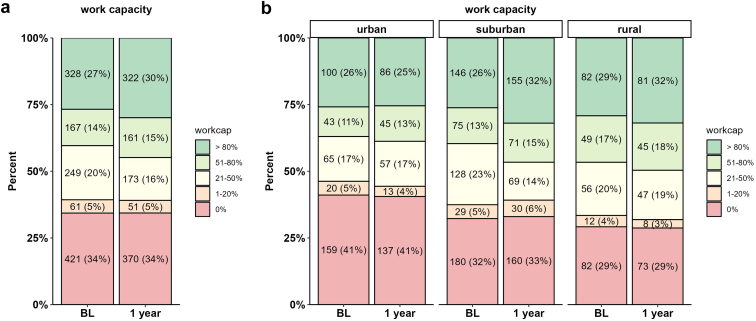
Methods: Retrospective, nationwide (Swiss Transplant Cohort Study [STCS]) study, from May 2008 to 2020, including 1926 patients aged 18 to 60 years who underwent KT. We investigated the self-reported work reintegration at 1, 3, and 5 years after the KT, the recipient and allograft survival, and the allograft function at 12 months, contingent on urbanization status (urban, suburban, rural).
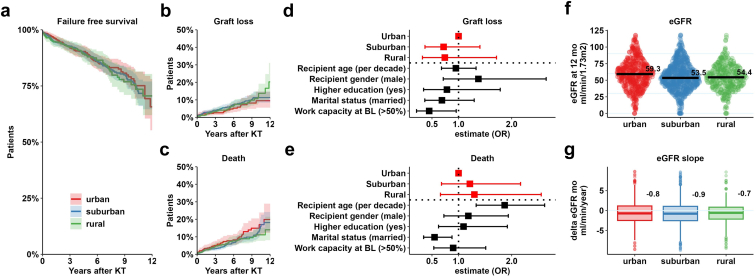
Results: The return rate of sufficiently filled-in questionnaires was 81% (1053 participants). Urban recipients were younger, had longer dialysis time before KT, and had less living donor KT. At baseline, the level of education, as well as the workforce defined as work capacity > 50%, were lower in urban areas (37% urban, 39% suburban, and 47% rural). Regression analysis revealed significantly higher odds ratio for employment 1 year post-KT among patients residing in rural and suburban areas (odds ratio: 1.31 [confidence interval: 1.04-1.65] and 1.52 [confidence interval: 1.16-1.98], respectively) compared to patients from urban regions. Stratified according to urbanization environment, recipient and allograft survival were comparable across groups.
Conclusion: Patient and graft outcomes were favorable, with improved work reintegration observed at the 1-year mark post-KT for recipients from rural backgrounds compared to those from suburban and urban areas.
Keywords: graft outcomes; kidney transplantation; urbanization; work capacity; work reintegration.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Geography About Switzerland. https://www.eda.admin.ch/aboutswitzerland/en/home/umwelt/geografie.html
-
- Boes S., Kaufmann C., Marti J. Sozioökonomische und kulturelle ungleichheiten im gesundheitsverhalten der Schweizer pevölkerung. 2016. https://www.obsan.admin.ch/de
-
- Cartier T., Senn N., Cornuz J., Bourgueil Y. In: Building Primary Care in a Changing Europe: Case Studies [Internet] Kringos D.S., Boerma W.G.W., Hutchinson A., et al., editors. European Observatory on Health Systems and Policies; 2015. Switzerland; pp. 275–283.https://www.ncbi.nlm.nih.gov/books/NBK459012/ Chapter 29 (Observatory Studies Series, No. 40) - PubMed
LinkOut - more resources
Full Text Sources
