

A multi-institutional retrospective cohort of adult-onset medulloblastoma in the modern era
- PMID: 39991182
- PMCID: PMC11842969
- DOI: 10.1093/noajnl/vdae231
A multi-institutional retrospective cohort of adult-onset medulloblastoma in the modern era
Abstract
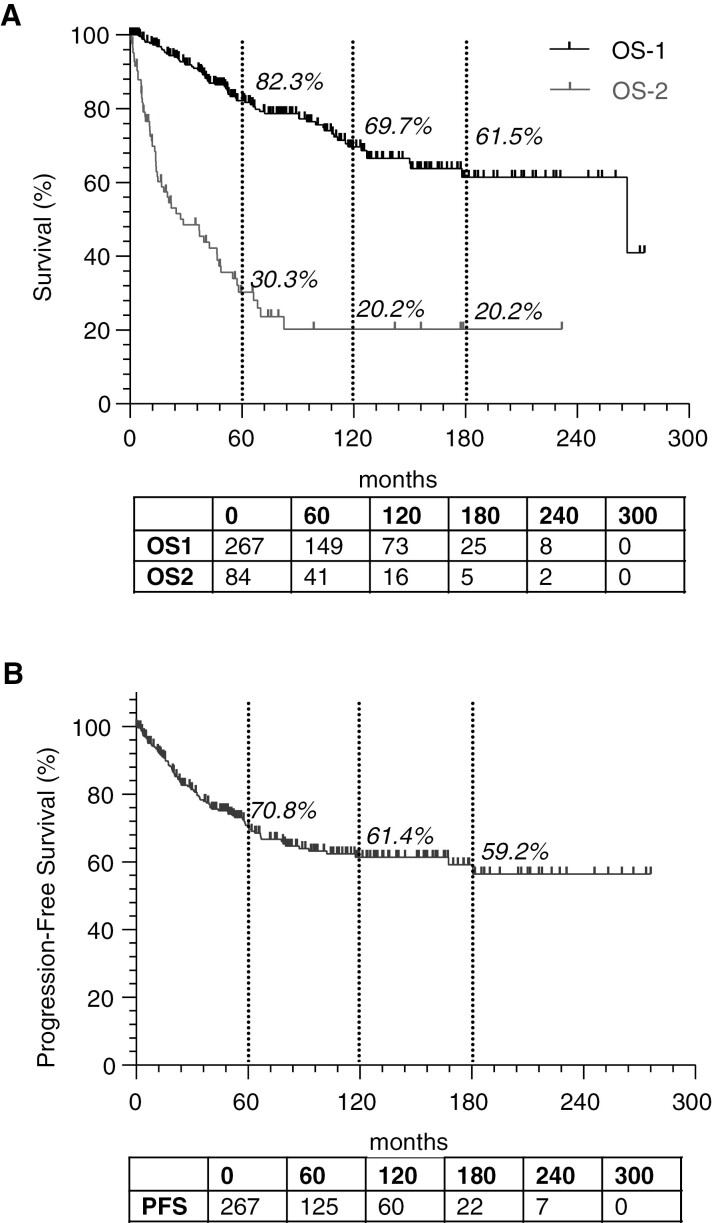
Background: Adult onset medulloblastoma (aMB) is a rare tumor with limited available evidence. We present a large multi-institutional retrospective cohort of aMB patients treated in the modern era, with an emphasis on understanding the role of chemotherapy at initial diagnosis.
Methods: We included 267 consecutive patients with aMB treated at 7 different institutions from 2000-present, controlling for chemotherapy regimen and cycles received.
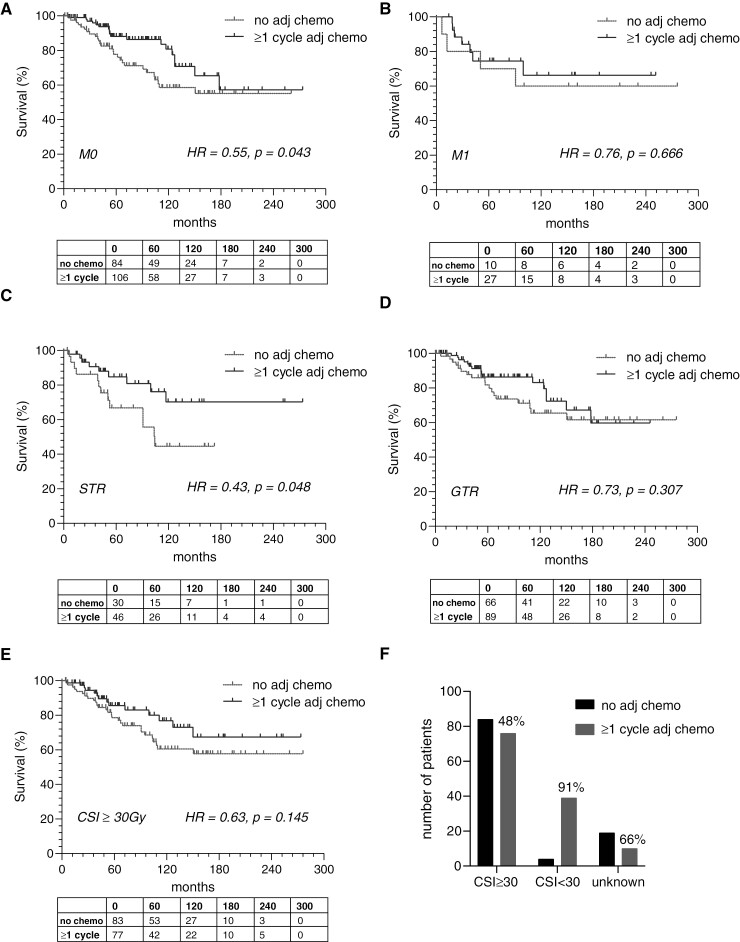
Results: Treatment factors were highly intercorrelated with one another and with treating institution. Concurrent chemotherapy was not associated with overall survival (OS). Adjuvant chemotherapy was associated with OS on univariable analyses (HR = 0.55, P = .029) and on multivariable analysis when adjusting for risk status (HR 0.55, P = .026) but not when also adjusting for treating institution. Proton craniospinal irradiation was associated with improved survival on univariable (HR = 0.50, P = .019) and multivariable analysis adjusting for risk status (HR = 0.51, P = .024) but not when treating institution was also considered. On subgroup analysis, adjuvant chemotherapy was associated with improved survival in M0 (HR = 0.55, P = .043) but not M1 disease, in patients with subtotal resection (HR = 0.43, P = .048) but not those with GTR. Similarly, progression-free survival was improved with chemotherapy in patients with M0 (HR = 0.57, P = .032) but not M1 disease, and in patients with subtotal (HR = 0.50, P = .054) but not gross total resection.
Conclusions: There was no benefit of concurrent chemotherapy. Adjuvant chemotherapy was associated with improved overall survival and this effect was driven by select subgroups, specifically those with M0 disease and those with residual tumor. We could not confirm that these associations are independent of the treating institution.
Keywords: adjuvant chemotherapy; adult medulloblastoma; concurrent chemotherapy; craniospinal radiation; proton.
© The Author(s) 2025. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
L.N.G.C. reports no relevant conflicts, but discloses consulting fees from Elsevier, Oakstone Publishing, BMJ Best Practice, and Servier. All other authors report no conflicts of interests or disclosures.
Figures
References
-
- Giordana MT, Schiffer P, Lanotte M, Girardi P, Chio A.. Epidemiology of adult medulloblastoma. Int J Cancer. 1999;80(5):689–692. - PubMed
-
- Smoll NR, Drummond KJ.. The incidence of medulloblastomas and primitive neurectodermal tumours in adults and children. J Clin Neurosci. 2012;19(11):1541–1544. - PubMed
-
- Remke M, Hielscher T, Northcott PA, et al.Adult medulloblastoma comprises three major molecular variants. J Clin Oncol. 2011;29(19):2717–2723. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources