

ANCA-Associated Glomerulonephritis: Diagnosis and Therapy Proceedings of the Henry Shavelle Lectureship
- PMID: 39991195
- PMCID: PMC11842095
- DOI: 10.1159/000542925
ANCA-Associated Glomerulonephritis: Diagnosis and Therapy Proceedings of the Henry Shavelle Lectureship
Abstract
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) frequently affects the kidney. Glomerulonephritis (GN) in AAV, ANCA-GN, not only dictates therapeutic decisions but is also of relevance for overall survival influencing the risk of cardiovascular disease and serious infections.
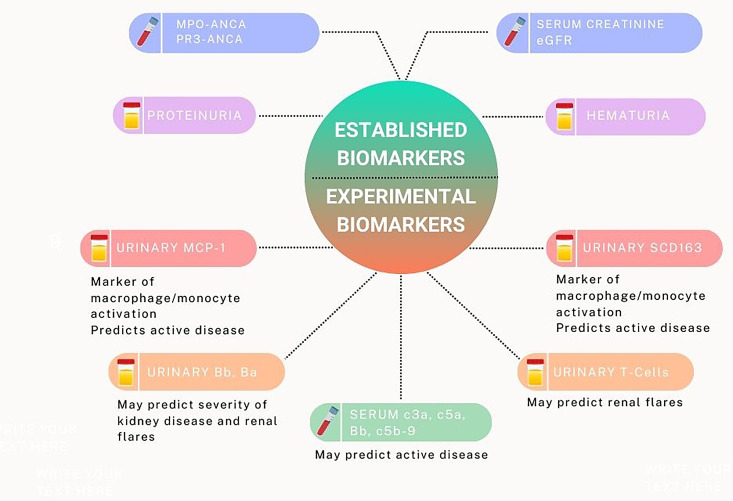
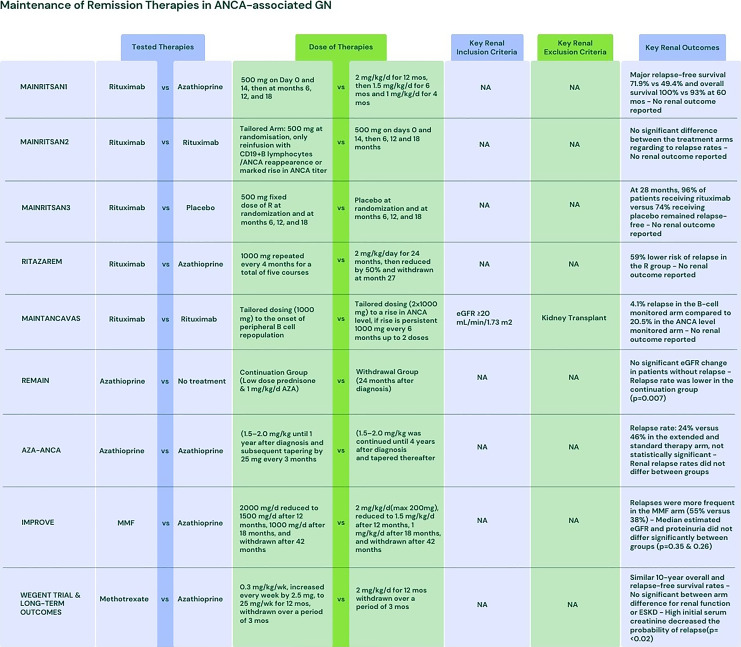
Summary: A diagnosis of ANCA-GN includes laboratory investigations including urinalysis and a thorough assessment of potential organ involvement. A kidney biopsy can be performed to ascertain the diagnosis but has an additional prognostic relevance and tools have been established to predict long-term kidney survival. Experimental biomarkers indicating kidney inflammation include urinary soluble CD163 and the presence of urinary T cells. Therapeutic options are refined and some of these therapies, such as the added value of performing plasma exchange, are the matter of controversial discussions. Safe reduction of cumulative exposure to glucocorticoids and eventually the use of avacopan to substantially reduce glucocorticoid exposure has been implemented in most centers. In the remission of maintenance, the optimal duration of therapy is still unclear, but extended use of rituximab as maintenance agent has shown long-term remission rates, thus limiting the damage accrued by relapsing disease and thus also reducing the risk of end-stage kidney disease (ESKD). Avacopan has been the first agent with a glomerular filtration rate-sparing effect, likely due to more rapid control of kidney inflammation. Those reaching ESKD should be evaluated for kidney transplantation and the risk of remaining on dialysis must be balanced against the risk of recurrence of disease following transplantation.
Key messages: The advent of a magnitude of landmark studies in ANCA-GN has refined diagnostic approaches, implemented tools to predict kidney outcome, and eventually led to the approval of newer therapies with avacopan, the latest addition to the armamentarium. Once ESKD is present, patients should be considered for kidney transplantation as remaining on dialysis portends poor overall prognosis.
Keywords: Anti-neutrophil cytoplasmic antibody; Diagnosis; Glomerulonephritis; Prognosis; Treatment.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Martin Windpessl received consulting and speaking fees from AstraZeneca, Boehringer Ingelheim, CSL Vifor, Delta 4, GlaxoSmithKline, Novartis, and Otsuka. Duvuru Geetha received consulting fees from Amgen, Calliditas, ChemoCentryx, Otsuka, and Vera Therapeutics. Ingeborg Bajema received consulting fees from Alentis, Amgen, Aurinia, CSL Vifor, GlaxoSmithKline, Hansa Biopharma, Novartis, Otsuka, and Vera Therapeutics. She is owner and director of BiPath. Sayna Norouzi received consulting fees from Boehringer Ingelheim, Calliditas, Novartis, and Otsuka. Andreas Kronbichler received grant support from CSL Vifor and consultancy fees from Amgen, AstraZeneca, Boehringer Ingelheim, CSL Vifor, Delta4, GlaxoSmithKline, Novartis, Novo Nordisk, Otsuka, Roche, Sobi, and Walden Biosciences. He serves as an associate editor of Glomerular Diseases and as an editor of Nephrology Dialysis Transplantation. Vanja Ivkovic, Ilay Berke, and Jasper Callemeyn declare no conflict of interests.
Figures
Similar articles
-
Plasma exchange and glucocorticoids to delay death or end-stage renal disease in anti-neutrophil cytoplasm antibody-associated vasculitis: PEXIVAS non-inferiority factorial RCT.Health Technol Assess. 2022 Sep;26(38):1-60. doi: 10.3310/PNXB5040. Health Technol Assess. 2022. PMID: 36155131 Clinical Trial.
-
Urinary Soluble CD163 and Disease Activity in Biopsy-Proven ANCA-Associated Glomerulonephritis.Clin J Am Soc Nephrol. 2020 Dec 7;15(12):1740-1748. doi: 10.2215/CJN.07210520. Epub 2020 Nov 17. Clin J Am Soc Nephrol. 2020. PMID: 33203735 Free PMC article.
-
Practical Management of ANCA-Associated Vasculitis: A Clinician's Perspective.Glomerular Dis. 2024 Dec 18;5(1):84-102. doi: 10.1159/000543159. eCollection 2025 Jan-Dec. Glomerular Dis. 2024. PMID: 39991192 Free PMC article.
-
Paediatric anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis: an update on renal management.Pediatr Nephrol. 2018 Jan;33(1):25-39. doi: 10.1007/s00467-016-3559-2. Epub 2017 Jan 6. Pediatr Nephrol. 2018. PMID: 28062909 Free PMC article. Review.
-
Diagnosing and treating ANCA-associated vasculitis: an updated review for clinical practice.Rheumatology (Oxford). 2023 May 2;62(5):1787-1803. doi: 10.1093/rheumatology/keac623. Rheumatology (Oxford). 2023. PMID: 36315063 Review.
Cited by
-
Malignancies and glomerulonephritis: when to suspect and when to screen?Clin Kidney J. 2025 Apr 10;18(5):sfaf101. doi: 10.1093/ckj/sfaf101. eCollection 2025 May. Clin Kidney J. 2025. PMID: 40352576 Free PMC article. Review.
References
-
- Kronbichler A, Shin JI, Lee KH, Nakagomi D, Quintana LF, Busch M, et al. . Clinical associations of renal involvement in ANCA-associated vasculitis. Autoimmun Rev. 2020;19(4):102495. - PubMed
-
- Gisslander K, White A, Aslett L, Hrušková Z, Lamprecht P, Musiał J, et al. . Data-driven subclassification of ANCA-associated vasculitis: model-based clustering of a federated international cohort. Lancet Rheumatol. 2024;6(11):e762–70. - PubMed
-
- Kronbichler A, Bajema IM, Bruchfeld A, Mastroianni Kirsztajn G, Stone JH. Diagnosis and management of ANCA-associated vasculitis. Lancet. 2024;403(10427):683–98. - PubMed
-
- Charles P, Perrodeau É, Samson M, Bonnotte B, Néel A, Agard C, et al. . Long-term rituximab use to maintain remission of antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med. 2020;173(3):179–87. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials