

Managing Bilateral Vernal Keratoconjunctivitis, Keratoconus, and Steroid-Induced Glaucoma: A Threefold Struggle
- PMID: 39991424
- PMCID: PMC11847309
- DOI: 10.7759/cureus.77901
Managing Bilateral Vernal Keratoconjunctivitis, Keratoconus, and Steroid-Induced Glaucoma: A Threefold Struggle
Abstract
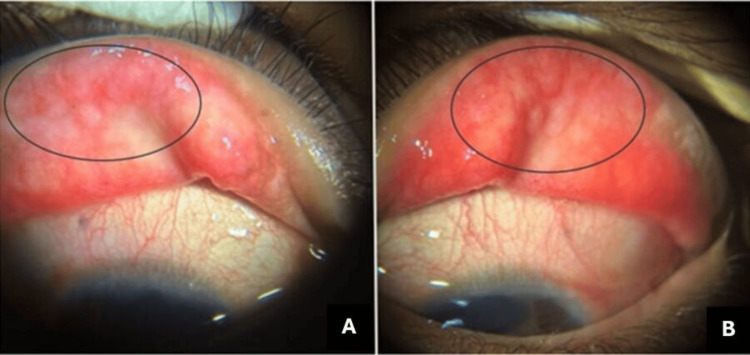
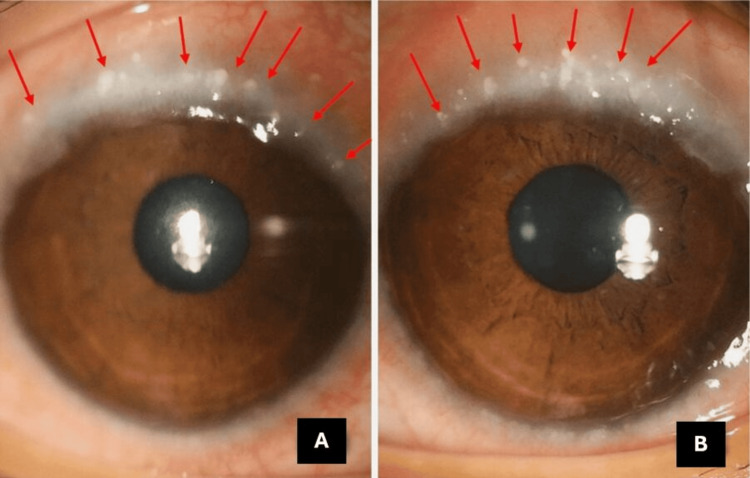
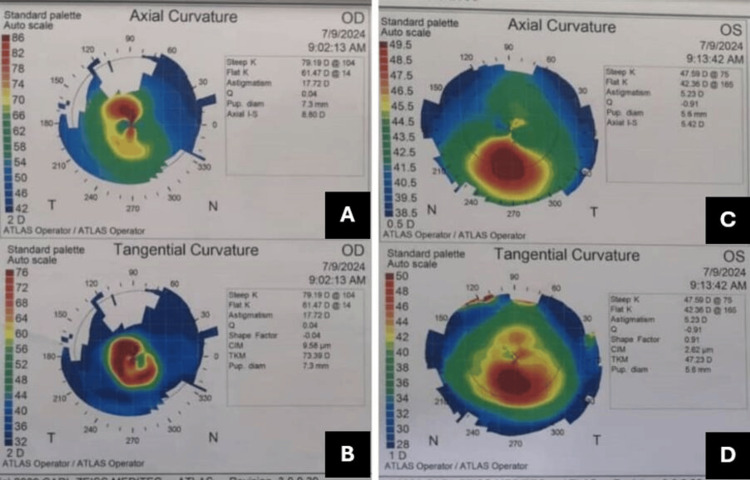
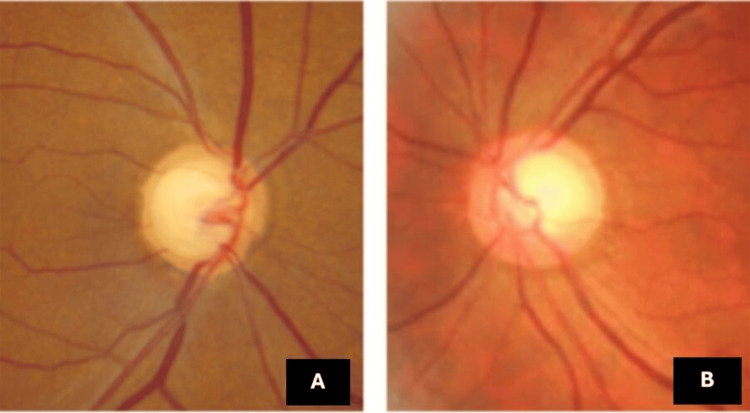
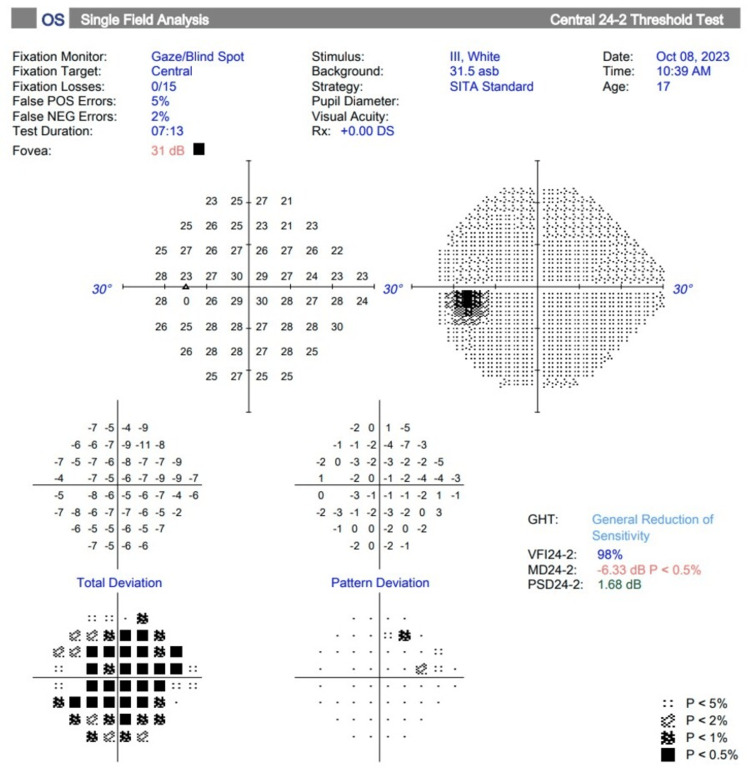
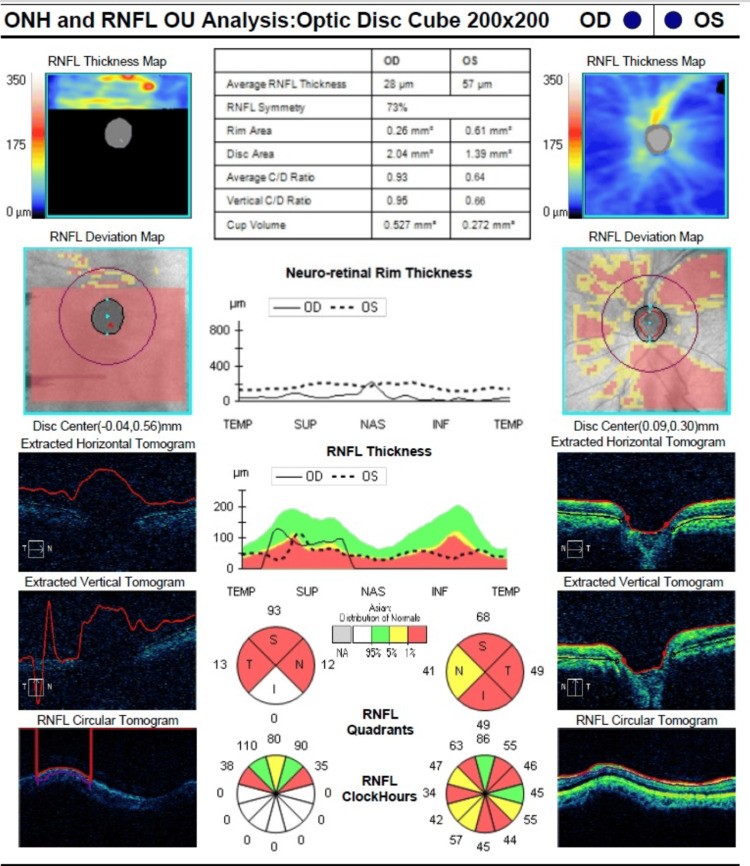
The coexistence of bilateral vernal keratoconjunctivitis (VKC), keratoconus, and steroid-induced glaucoma presents a complex ocular challenge, threatening visual acuity and long-term eye health. This combination poses significant risks, with VKC and keratoconus progressively affecting both eyes while glaucoma, induced by necessary steroid treatments, further complicates the clinical picture. We report a case of a young Malay girl who complained of bilateral eye itchiness with progressive blurring of vision, a history of frequent changes in prescribed glasses, and vigorous eye rubbing. Diagnosed with VKC at age 14, she defaulted on follow-up and began unsupervised use of topical steroids during flare-ups. This resulted in steroid-induced glaucoma, complicating the management of both VKC and coexisting keratoconus. This case underscores the importance of careful, supervised treatment, as improper management can significantly affect long-term outcomes.
Keywords: corticosteriod; flare-up; keratoconus (kc); steroid-induced glaucoma; vernal keratoconjunctivitis.
Copyright © 2025, Maffar et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Treating refractory corneal hydrops in a male patient with vernal keratoconjunctivitis and mental retardation: a case report.BMC Ophthalmol. 2022 Jan 24;22(1):36. doi: 10.1186/s12886-021-02241-6. BMC Ophthalmol. 2022. PMID: 35073856 Free PMC article.
-
Ocular complications of severe vernal keratoconjunctivitis (VKC) in Yemen.Saudi J Ophthalmol. 2011 Jul;25(3):291-4. doi: 10.1016/j.sjopt.2011.02.001. Epub 2011 Feb 16. Saudi J Ophthalmol. 2011. PMID: 23960939 Free PMC article.
-
The effect of vernal keratoconjunctivitis on clinical outcomes of penetrating keratoplasty for keratoconus.Can J Ophthalmol. 2004 Dec;39(7):772-7. doi: 10.1016/s0008-4182(04)80072-3. Can J Ophthalmol. 2004. PMID: 15696768
-
Vernal keratoconjunctivitis and keratoconus.Curr Opin Allergy Clin Immunol. 2021 Oct 1;21(5):507-514. doi: 10.1097/ACI.0000000000000765. Curr Opin Allergy Clin Immunol. 2021. PMID: 34269743 Review.
-
Vernal keratoconjunctivitis: a severe allergic eye disease with remodeling changes.Pediatr Allergy Immunol. 2014 Jun;25(4):314-22. doi: 10.1111/pai.12197. Epub 2014 Jan 20. Pediatr Allergy Immunol. 2014. PMID: 24438133 Review.
References
-
- A review of four hundred cases of vernal conjunctivitis. Neumann E, Gutmann MJ, Blumenkrantz N, Michaelson IC. Am J Ophthalmol. 1959;47:166–172. - PubMed
Publication types
LinkOut - more resources
Full Text Sources