

Heart failure with supranormal ejection fraction: clinical characteristics and outcomes compared to mildly reduced and preserved ejection fraction
- PMID: 39992387
- PMCID: PMC12058924
- DOI: 10.1007/s00392-025-02620-9
Heart failure with supranormal ejection fraction: clinical characteristics and outcomes compared to mildly reduced and preserved ejection fraction
Abstract
Background: Little is known about the recently emerging entity, heart failure with supranormal ejection fraction (HFsnEF).
Objective: To describe the clinical characteristics and outcome of HFsnEF, compared to HF with mildly reduced EF (HFmrEF) and HF with preserved EF (HFpEF) patients.
Design: A single center retrospective analysis.
Patients: Hospitalized and ambulatory heart failure (HF) patients who underwent echocardiography with left ventricular ejection fraction (LVEF) > 40%.
Main measures: Clinical and echocardiographic parameters, hospitalization rates and mortality.
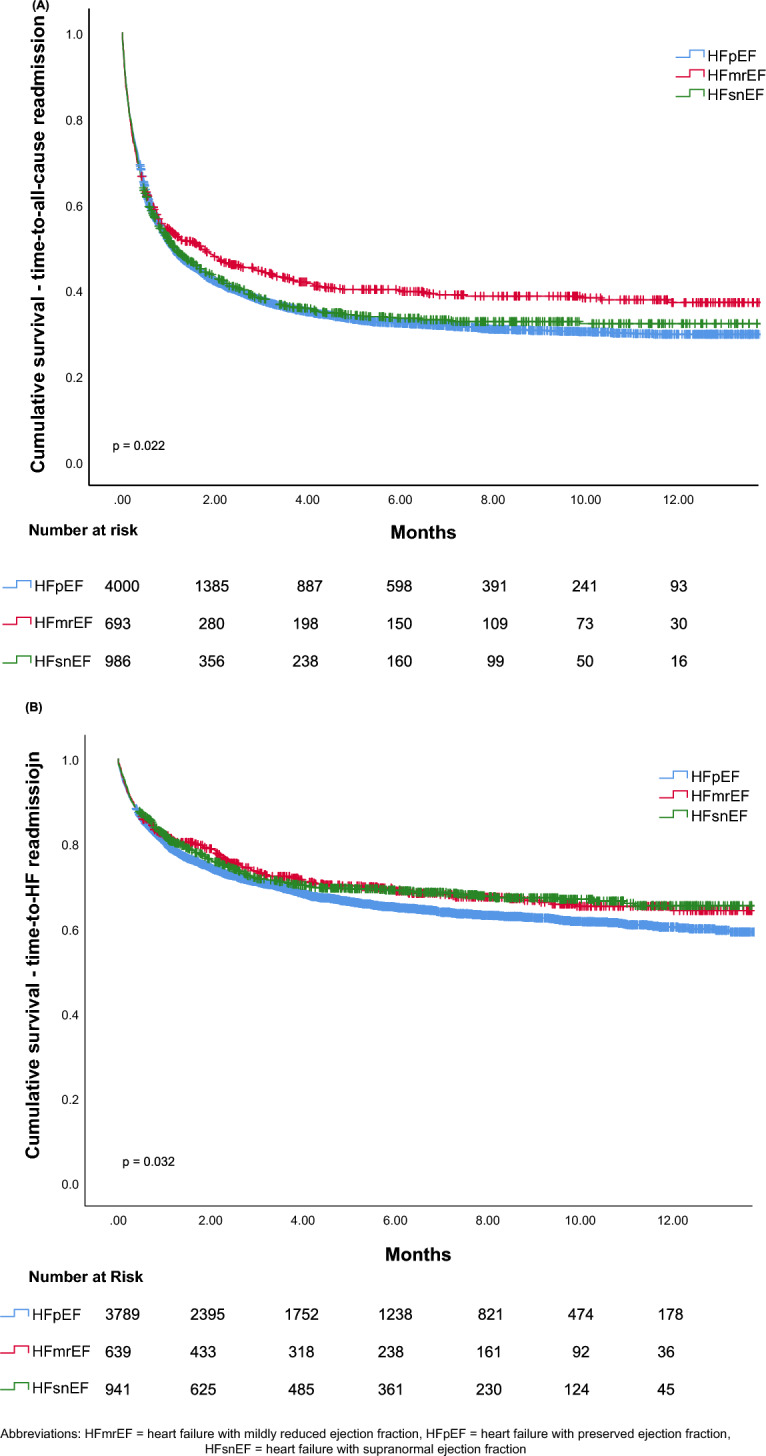
Key results: A total of 6,202 patients (mean age 81.4 ± 14.1 years, 52% females) were analyzed: 750 in the HFmrEF group (LVEF 41-49%), 4360 in the HFpEF group (LVEF 50-64%), and 1092 in the HFsnEF group (LVEF ≥ 65%). Patients were followed for a median of 32 (11-65) months. HFsnEF patients were older, predominantly female, exhibited higher hypertension prevalence, more severe LV hypertrophy, smaller LV dimensions, and higher filling pressures compared to the other groups (p < 0.001 for all). These features were consistent in both hospitalized and ambulatory patients. In a univariable model, HFsnEF patients had higher mortality rates compared to HFmrEF and HFpEF patients (HR 1.258, 95% CI 1.117-1.418; p < 0.001 and HR 1.112, 95% CI 1.023-1.208; p = 0.012, respectively). However, in a multivariable model, adjusted for age, sex, comorbidities, and echocardiographic parameters, there was no significant difference in the mortality rates between all groups. The total hospitalization rate was similar between the HFpEF and HFsnEF groups, and lower in the HFmrEF group (p = 0.022). However, the HFsnEF group had the lowest rate of HF-related hospitalizations (p = 0.002).
Conclusion: HFsnEF represents a group of patients with a distinct clinical and echocardiographic profile accompanied by worse outcomes, likely mediated by older age and a higher comorbidity burden, compared to HFmrEF and HFpEF. Therefore, the supranormal EF may serve as a marker rather than an independent prognostic factor.
Keywords: Characteristics; HFsnEF; Outcomes; Prognosis; Supranormal EF.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no relevant financial or non-financial interests to disclose. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Sheba Medical Center (SMC-9148-22).
Figures

References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Members: AF et al (2021) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Heart Fail 24(1):4–131. 10.1002/ejhf.2333 - PubMed
-
- Flack JM, Adekola B (2020) Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc Med 30(3):160–164 - PubMed
-
- Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP et al (2019) Angiotensin-Neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med 381(17):1609–1620 - PubMed
-
- Lund LH, Claggett B, Liu J, Lam CS, Jhund PS, Rosano GM et al (2018) Heart failure with mid-range ejection fraction in CHARM: characteristics, outcomes and effect of candesartan across the entire ejection fraction spectrum. Eur J Heart Fail 20(8):1230–1239 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
