

Nilotinib attenuates vascular pathology in experimental cerebral malaria
- PMID: 39993234
- PMCID: PMC12143834
- DOI: 10.1182/bloodadvances.2024015364
Nilotinib attenuates vascular pathology in experimental cerebral malaria
Abstract
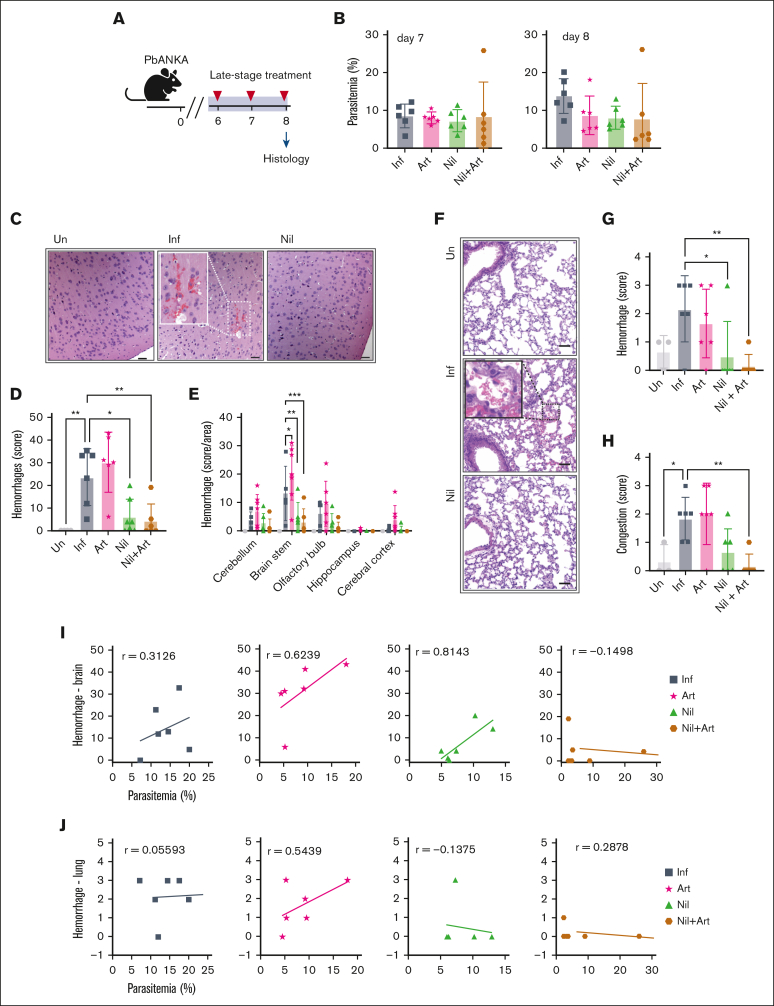
Cerebral malaria (CM), a life-threatening complication of Plasmodium falciparum infection, is characterized by the sequestration of infected erythrocytes in the brain microvasculature. Our study investigated the potential of repurposing tyrosine kinase inhibitors targeting BCR-ABL1 (BCR-ABL drugs), which are also known to be effective against P falciparum blood-stage parasites, for mitigating inflammation and blood-brain barrier breakdown in CM. Our analysis demonstrated differential protective effects of BCR-ABL drugs on primary human brain microvascular endothelial cells exposed to thrombin or a P falciparum-infected erythrocyte challenge. Bosutinib attenuated both thrombin- and parasite-induced barrier alterations, whereas nilotinib was only effective against thrombin, and imatinib protected against neither. Bosutinib's barrier protective effect was associated with reduced interendothelial gap formation and decreased phosphorylation of the adherens junction protein VE-cadherin and the focal adhesion protein paxillin. In the mouse experimental CM model, nilotinib showed superior efficacy over imatinib and bosutinib. In mice, nilotinib led to fewer brain hemorrhages and less vascular congestion than the antimalaria drug artesunate at similar levels of parasitemia control. Our findings provide important mechanistic insight into the activities of BCR-ABL drugs to suppress endothelial barrier disruptive signaling in vitro and to protect in a mouse model of CM. These findings can inform the repurposing of these drugs in malaria treatment, particularly for managing cerebral complications.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures







References
-
- Lee WL, Slutsky AS. Sepsis and endothelial permeability. N Engl J Med. 2010;363(7):689–691. - PubMed
-
- World Malaria Report 2022. Global Malaria Programme; 2022.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
