

Individual bioenergetic capacity as a potential source of resilience to Alzheimer's disease
- PMID: 39994231
- PMCID: PMC11850607
- DOI: 10.1038/s41467-025-57032-0
Individual bioenergetic capacity as a potential source of resilience to Alzheimer's disease
Abstract
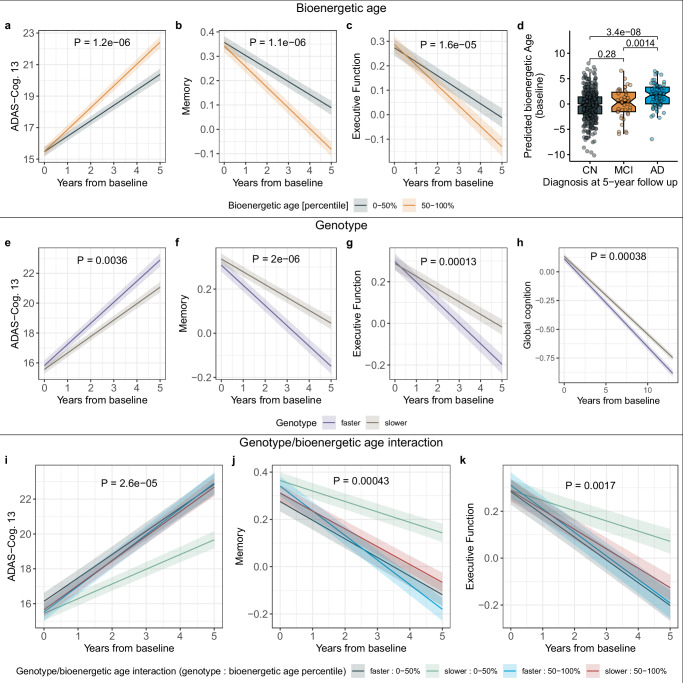
Impaired glucose uptake in the brain is an early presymptomatic manifestation of Alzheimer's disease (AD), with symptom-free periods of varying duration that likely reflect individual differences in metabolic resilience. We propose a systemic "bioenergetic capacity", the individual ability to maintain energy homeostasis under pathological conditions. Using fasting serum acylcarnitine profiles from the AD Neuroimaging Initiative as a blood-based readout for this capacity, we identified subgroups with distinct clinical and biomarker presentations of AD. Our data suggests that improving beta-oxidation efficiency can decelerate bioenergetic aging and disease progression. The estimated treatment effects of targeting the bioenergetic capacity were comparable to those of recently approved anti-amyloid therapies, particularly in individuals with specific mitochondrial genotypes linked to succinylcarnitine metabolism. Taken together, our findings provide evidence that therapeutically enhancing bioenergetic health may reduce the risk of symptomatic AD. Furthermore, monitoring the bioenergetic capacity via blood acylcarnitine measurements can be achieved using existing clinical assays.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.J.S. is a member of the Scientific Advisory Board of Bayer Oncology and of the Dementia Advisory Board of Siemens Medical Solutions USA, Inc.; A.J.S received in-kind support from Avid Radiopharmaceuticals, a subsidiary of Eli Lilly (PET tracer precursor); A.J.S. received Editorial Office Support as Editor-in-Chief from Springer-Nature Publishing (Brain Imaging and Behavior). P.M.D. has received research grants (through Duke University) from Lilly, Avanir, Bausch, Alzheimer’s Drug Discovery Foundation; P.M.D. has received advisory fees from Verily, Otsuka, Genomind, Cogniciti, Clearview, VitaKey, Neuronix, Neuroglee, and Transposon Therapeutics; P.M.D. owns shares or options in UMethod, Evidation Health, Transposon, Marvel Biome, and Advera Health; P.M.D. serves on the board of Apollo and is a co-inventor (through Duke University) on patents relating to dementia biomarkers, metabolomics, and therapies. R.K.D holds equity in Metabolon Inc. M.A., R.K.D., and G.K. are co-inventors (through Duke University/Helmholtz Zentrum München) on patents on applications of metabolomics in diseases of the central nervous system; M.A., R.K.D., G.K., and J.K. hold equity in Chymia LLC and IP in PsyProtix/atai Life Sciences N.V. that are exploring the potential for therapeutic applications targeting mitochondrial metabolism in treatment-resistant depression. JK is a confounder of iollo, advisor to Everfur, and advisor/part-time employee at ExactRx. The remaining authors declare no competing interests.
Figures



Update of
-
Individual bioenergetic capacity as a potential source of resilience to Alzheimer's disease.medRxiv [Preprint]. 2024 Jan 24:2024.01.23.23297820. doi: 10.1101/2024.01.23.23297820. medRxiv. 2024. Update in: Nat Commun. 2025 Feb 24;16(1):1910. doi: 10.1038/s41467-025-57032-0. PMID: 38313266 Free PMC article. Updated. Preprint.
References
-
- Heiss, W. D. et al. Positron emission tomography findings in dementia disorders: contributions to differential diagnosis and objectivizing of therapeutic effects. Keio J. Med.38, 111–135 (1989). - PubMed
-
- Heiss, W. D., Szelies, B., Kessler, J. & Herholz, K. Abnormalities of energy metabolism in Alzheimer’s disease studied with PET. Ann. N. Y. Acad. Sci.640, 65–71 (1991). - PubMed
-
- Kessler, J., Herholz, K., Grond, M. & Heiss, W. D. Impaired metabolic activation in Alzheimer’s disease: a PET study during continuous visual recognition. Neuropsychologia29, 229–243 (1991). - PubMed
MeSH terms
Substances
Grants and funding
- P30 AG072975/AG/NIA NIH HHS/United States
- N01 AG012100/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- U19 AG063744/AG/NIA NIH HHS/United States
- R01 AG032990/AG/NIA NIH HHS/United States
- R01 NS080820/NS/NINDS NIH HHS/United States
- RC2 AG036547/AG/NIA NIH HHS/United States
- U01 AG061359/AG/NIA NIH HHS/United States
- P01 AG017216/AG/NIA NIH HHS/United States
- R01 AG046171/AG/NIA NIH HHS/United States
- U01 AG046152/AG/NIA NIH HHS/United States
- U01 AG061356/AG/NIA NIH HHS/United States
- U01 AG032984/AG/NIA NIH HHS/United States
- R01 AG030146/AG/NIA NIH HHS/United States
- U01 AG024904/AG/NIA NIH HHS/United States
- R01 AG069901/AG/NIA NIH HHS/United States
- R01 AG017917/AG/NIA NIH HHS/United States
- R01 AG036042/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- RF1 AG059093/AG/NIA NIH HHS/United States
- RF1 AG057473/AG/NIA NIH HHS/United States
- U01 AG046139/AG/NIA NIH HHS/United States
- P01 AG003949/AG/NIA NIH HHS/United States
- U01 AG046161/AG/NIA NIH HHS/United States
- R01 AG048015/AG/NIA NIH HHS/United States
- P50 AG025711/AG/NIA NIH HHS/United States
- RF1 AG058942/AG/NIA NIH HHS/United States
- HHSN271201200022C/DA/NIDA NIH HHS/United States
- RF1 AG051550/AG/NIA NIH HHS/United States
- R01 AG018023/AG/NIA NIH HHS/United States
- U01 AG006786/AG/NIA NIH HHS/United States
- R01 AG036836/AG/NIA NIH HHS/United States
- R01 AG015819/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
