

On-patient medical record and mRNA therapeutics using intradermal microneedles
- PMID: 39994390
- PMCID: PMC12048341
- DOI: 10.1038/s41563-024-02115-4
On-patient medical record and mRNA therapeutics using intradermal microneedles
Abstract
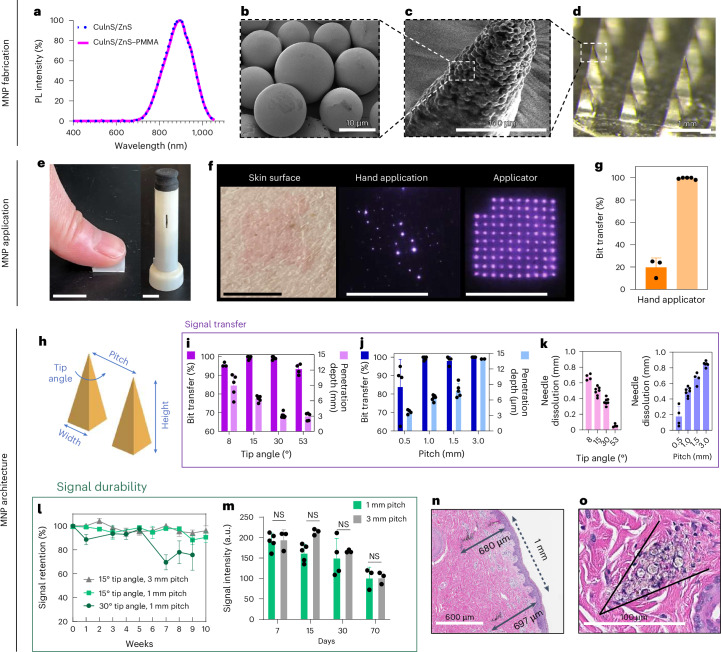
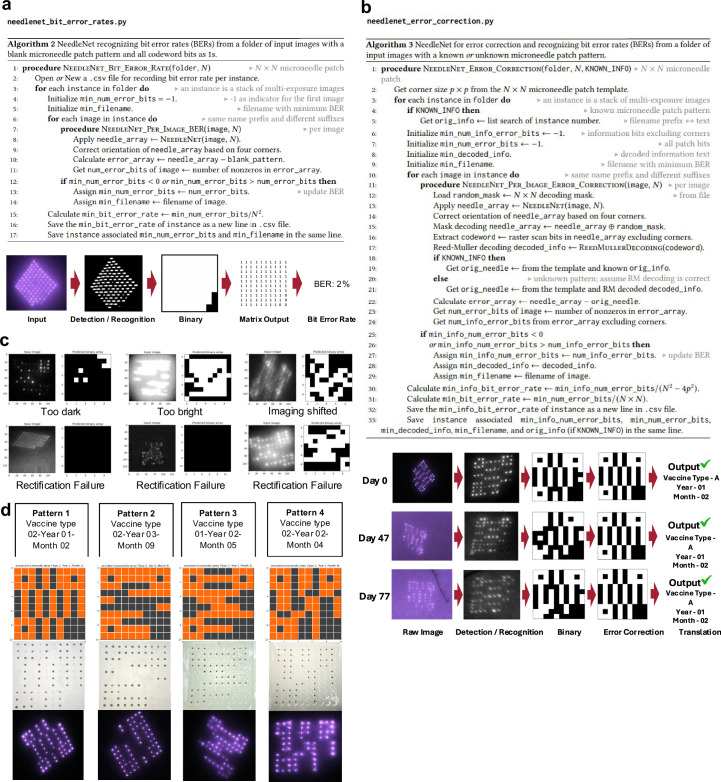
Medical interventions often require timed series of doses, thus necessitating accurate medical record-keeping. In many global settings, these records are unreliable or unavailable at the point of care, leading to less effective treatments or disease prevention. Here we present an invisible-to-the-naked-eye on-patient medical record-keeping technology that accurately stores medical information in the patient skin as part of microneedles that are used for intradermal therapeutics. We optimize the microneedle design for both a reliable delivery of messenger RNA (mRNA) therapeutics and the near-infrared fluorescent microparticles that encode the on-patient medical record-keeping. Deep learning-based image processing enables encoding and decoding of the information with excellent temporal and spatial robustness. Long-term studies in a swine model demonstrate the safety, efficacy and reliability of this approach for the co-delivery of on-patient medical record-keeping and the mRNA vaccine encoding severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This technology could help healthcare workers make informed decisions in circumstances where reliable record-keeping is unavailable, thus contributing to global healthcare equity.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: R.L. is a founder and board member of Moderna. A list of entities with which R.L. is involved, compensated or uncompensated, is in Supplementary Note 1. A list of entities with which A.J. is involved, or has been recently involved, compensated or uncompensated, is in Supplementary Note 2. The other authors declare no competing interests.
Figures













References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
