

Antidepressant use and cognitive decline in patients with dementia: a national cohort study
- PMID: 39994788
- PMCID: PMC11854023
- DOI: 10.1186/s12916-025-03851-3
Antidepressant use and cognitive decline in patients with dementia: a national cohort study
Abstract
Background: Dementia is associated with psychiatric symptoms but the effects of antidepressants on cognitive function in dementia are understudied. We aimed to investigate the association between antidepressants and cognitive decline in patients with dementia, and the risk of severe dementia, fractures and death, depending on antidepressant class, drug, and dose.
Methods: This is a national cohort study. Patients with dementia registered in the Swedish Registry for Cognitive/Dementia Disorders-SveDem from May 1, 2007, until October 16, 2018, with at least one follow-up after dementia diagnosis, and who were new users of antidepressants, were included. Antidepressant use as a time varying exposure defined during the 6 months leading up to dementia diagnosis or each subsequent follow-up. We used linear mixed models to examine the association between antidepressant use and cognitive trajectories assessed by Mini-Mental State Examination (MMSE) scores. We used Cox proportional hazards models to calculate the hazard ratios for severe dementia (MMSE score < 10), fracture, and death. We compared antidepressant classes and drugs, and analyzed dose-response.
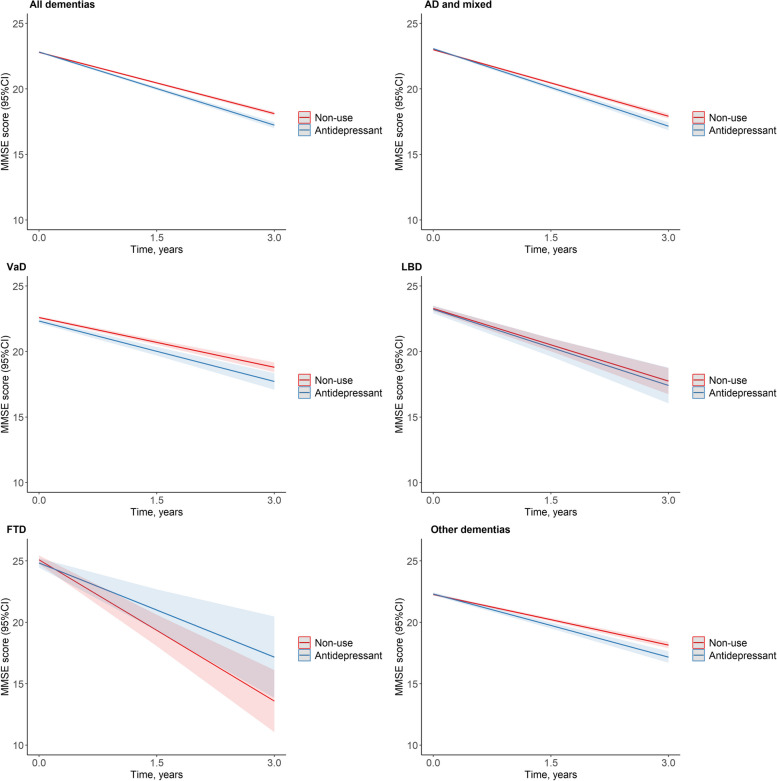
Results: We included 18740 patients (10 205 women [54.5%]; mean [SD] age, 78.2[7.4] years), of which 4271 (22.8%) received at least one prescription for an antidepressant. During follow-up, a total of 11912 prescriptions for antidepressants were issued, with selective serotonin reuptake inhibitors (SSRI) being the most common (64.8%). Antidepressant use was associated with faster cognitive decline (β (95% CI) = - 0.30(- 0.39, - 0.21) points/year), in particular sertraline (- 0.25(- 0.43, - 0.06) points/year), citalopram (- 0.41(- 0.55, - 0.27) points/year), escitalopram (- 0.76(- 1.09, - 0.44) points/year), and mirtazapine (- 0.19(- 0.34, - 0.04) points/year) compared with non-use. The association was stronger in patients with severe dementia (initial MMSE scores 0-9). Escitalopram showed a greater decline rate than sertraline. Compared with non-use, dose response of SSRIs on greater cognitive decline and higher risks of severe dementia, all-cause mortality, and fracture were observed.
Conclusions: In this cohort study, current antidepressant use was associated with faster cognitive decline; furthermore, higher dispensed doses of SSRIs were associated with higher risk for severe dementia, fractures, and all-cause mortality. These findings highlight the significance of careful and regular monitoring to assess the risks and benefits of different antidepressants use in patients with dementia.
Keywords: Antidepressants; Cognitive decline; Cohort; Dementia; Mortality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The requirement of written consent for this study was waived due to the register data being pseudonymized before delivery to our research group. The regional ethics committee in Stockholm approved the study (dnr 2017/501–31; 2017/942–32), which complies with the Declaration of Helsinki 31. Participants and caretakers are informed verbally about SveDem and could decline participation. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Tampi RR, Jeste DV. Dementia Is More Than Memory Loss: Neuropsychiatric Symptoms of Dementia and Their Nonpharmacological and Pharmacological Management. Am J Psychiatry. 2022;179(8):528–43. - PubMed
-
- Blumberg MJ, Vaccarino SR, McInerney SJ. Procognitive Effects of Antidepressants and Other Therapeutic Agents in Major Depressive Disorder: A Systematic Review. J Clin Psychiatry. 2020;81(4). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
