

Systemic Inflammation and the Inflammatory Context of the Colonic Microenvironment Are Improved by Urolithin A
- PMID: 39995164
- PMCID: PMC11979956
- DOI: 10.1158/1940-6207.CAPR-24-0383
Systemic Inflammation and the Inflammatory Context of the Colonic Microenvironment Are Improved by Urolithin A
Abstract
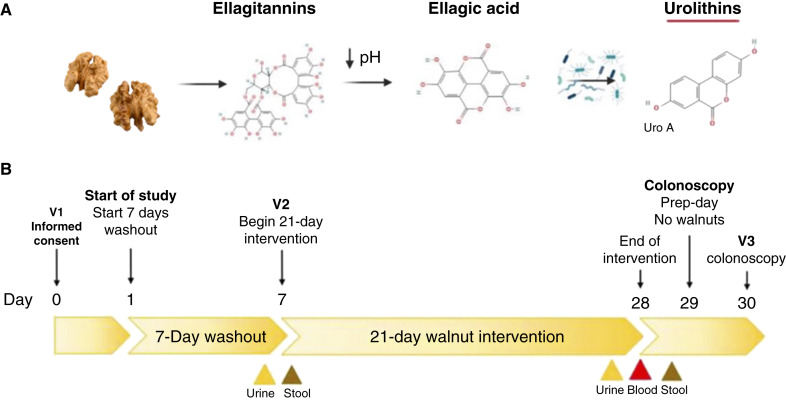
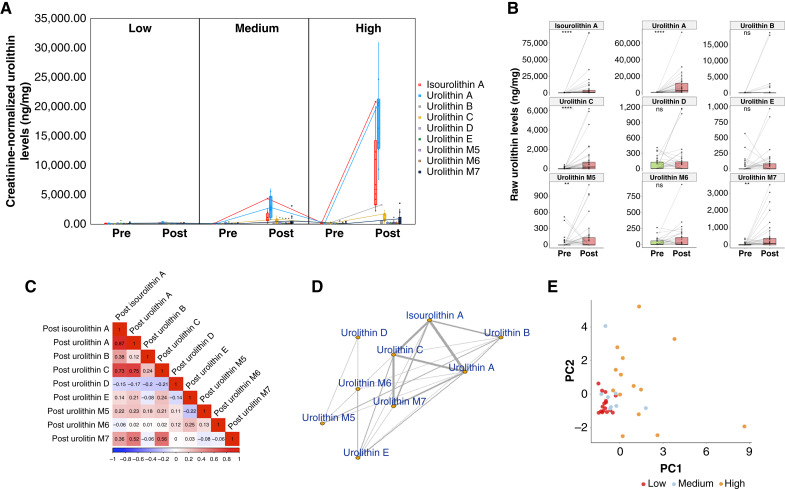
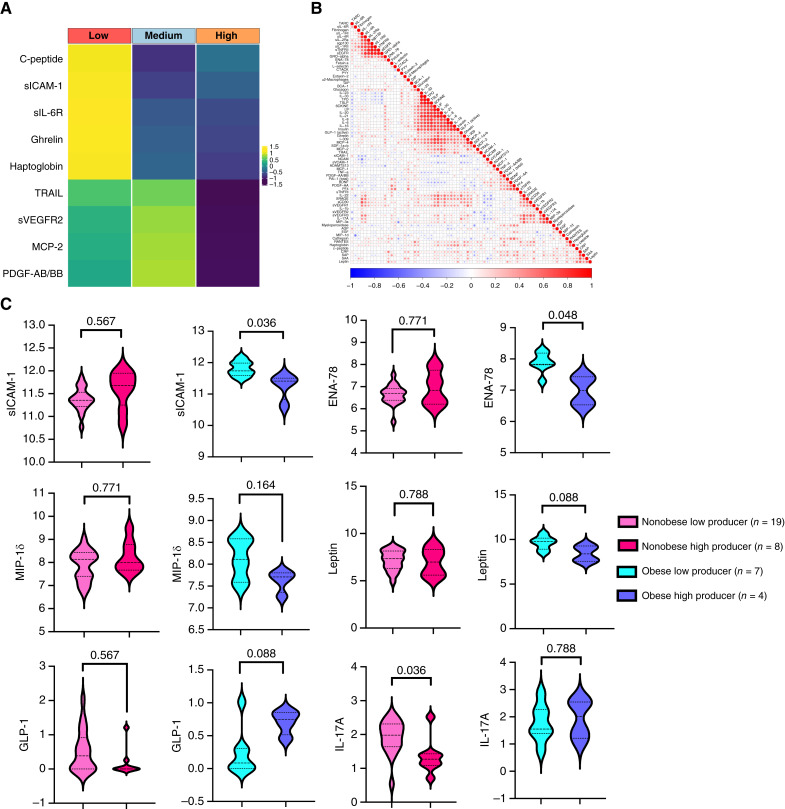
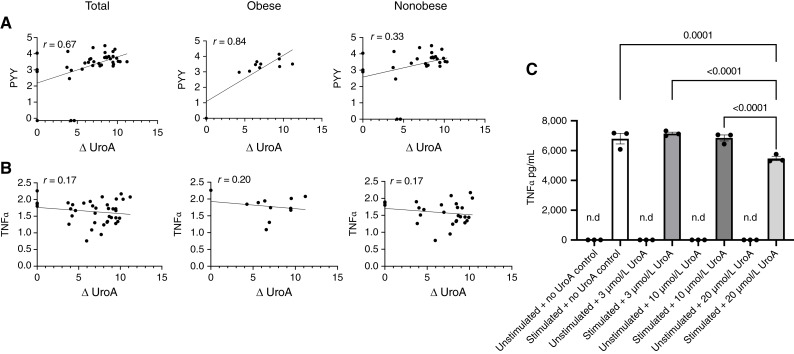
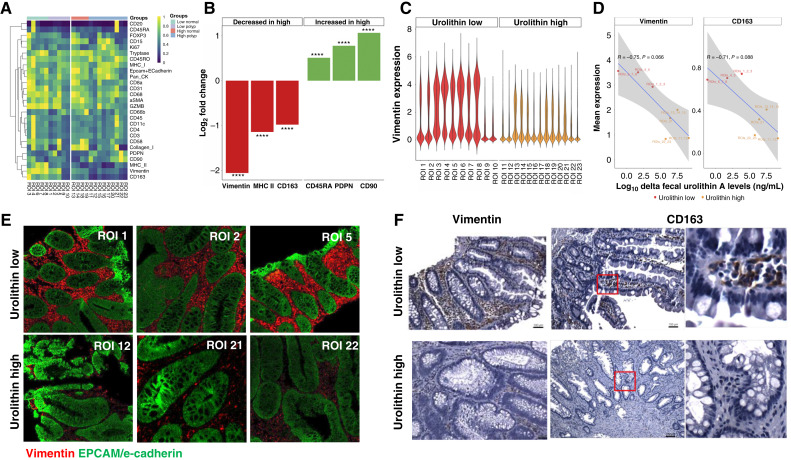
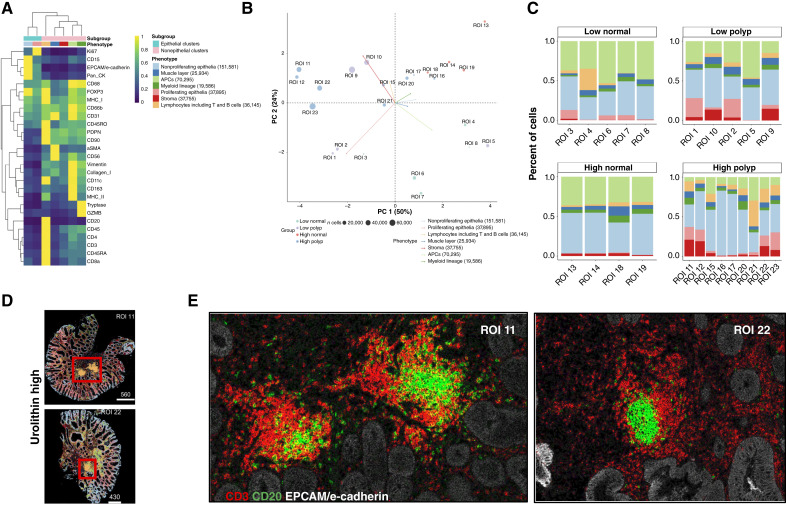
Diet affects cancer risk, and plant-derived polyphenols exhibit cancer-preventive properties. Walnuts are an exceptional source of polyphenolic ellagitannins, converted into urolithins by gut microflora. This clinical study examines the impact of urolithin metabolism on inflammatory markers in blood and colon polyp tissue. We evaluate the effects of walnut consumption on urinary urolithins, serum inflammatory markers, and immune cell markers in polyp tissues obtained from 39 subjects. Together with detailed food frequency data, we perform integrated computational analysis of metabolomic data combined with serum inflammatory markers and spatial imaging of polyp tissues using imaging mass cytometry. LC/MS-MS analyses of urine and fecal samples identify a widely divergent capacity to form nine urolithin metabolites in this patient population. Subjects with higher urolithin A formation exhibit lower levels of several key serologic inflammatory markers, including C-peptide, soluble form of intracellular adhesion molecule 1, sIL-6R, ghrelin, TRAIL, sVEGFR2, platelet-derived growth factor (PDGF), and MCP-2, alterations that are more pronounced in obese individuals for soluble form of intracellular adhesion molecule 1, epithelial neutrophil-activating peptide 78, leptin, glucagon-like peptide 1, and macrophage inflammatory protein 1δ. There is a significant increase in levels of peptide YY associated with urolithin A formation, whereas TNFα levels show an opposite trend, recapitulated in an in vitro system with ionomycin/phorbol 12-myristate 13-acetate-stimulated peripheral blood mononuclear cells (PBMC). Spatial imaging of colon polyp tissues shows altered cell cluster patterns, including a significant reduction of vimentin and CD163 expression associated with urolithin A. The ability to form urolithin A is linked to inflammation, warranting further studies to understand the role of urolithins in cancer prevention. Prevention Relevance: We evaluate cancer-protective effects of walnuts via formation of microbe-derived urolithin A, substantiating their functional benefits on serum inflammatory markers and immunologic composition of polyps in normal/obese subjects. Our approach incorporates personalized nutrition within the context of colonic health, providing the rationale for dietary inclusion of walnut ellagitannins for cancer prevention.
©2025 American Association for Cancer Research.
Conflict of interest statement
A. Aksenov reports being a co-founder of Arome Science, Inc. and Bileomix, Inc. V.N. Motta reports other support from Standard BioTools during the conduct of the study, as well as other support from Standard BioTools outside the submitted work. No disclosures were reported by the other authors.
Figures

References
-
- Denk D, Petrocelli V, Conche C, Drachsler M, Ziegler PK, Braun A, et al. Expansion of T memory stem cells with superior anti-tumor immunity by Urolithin A-induced mitophagy. Immunity 2022;55:2059–73.e8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
