

Status of cerebrovascular autoregulation relates to outcome in severe paediatric head injury: STARSHIP, a prospective multicentre validation study
- PMID: 39996125
- PMCID: PMC11848105
- DOI: 10.1016/j.eclinm.2025.103077
Status of cerebrovascular autoregulation relates to outcome in severe paediatric head injury: STARSHIP, a prospective multicentre validation study
Abstract
Background: Continuous assessment of cerebral autoregulation (CA) using pressure reactivity index (PRx), is a promising tool for individualized management to improve outcome after traumatic brain injury (TBI). However, experience with CA in paediatric TBI (pTBI) is limited to retrospective or single-centre studies.
Methods: Studying Trends of AutoRegulation in Severe Head Injury in Paediatrics (STARSHIP) (clinicalTrials.gov identifier-NCT0688462), was a prospective, multicentre, observational, research database study conducted across 10 identified UK Paediatric Intensive Care Units from 01.07.2018 till 31.04.2024. The main objective was to validate and identify optimal thresholds of PRx associated with outcome (as assessed with Glasgow outcome scale extended for Pediatrics at 12 months) in children (<16 years) requiring invasive arterial blood pressure and intracranial pressure monitoring for TBI and establish a comprehensive research database. Apart from high-resolution data, clinical and outcome data up to 12 months post-ictus were collected. Univariable and multivariable analyses including propensity score matching, were employed to determine the effect of PRx on outcome whilst considering covariates, centre-specific differences and other multimodal metrics.
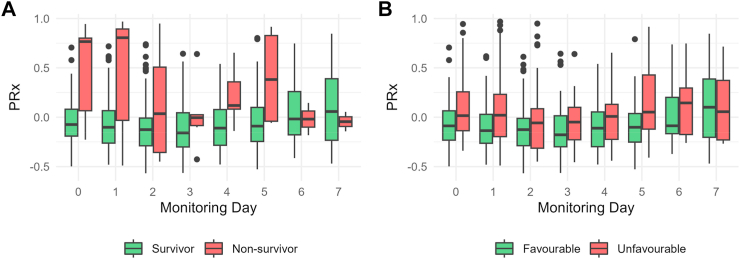
Findings: Out of 153 recruited, 135 children (median age 96 months) with consent and adequate data were included. Overall median PRx of the cohort was -0.09 (IQR -0.19 to 0.08). Both ICP and PRx were elevated in non-survivors and children with unfavourable outcome. PRx retained a significant effect on outcome after adjusting for various clinical and monitoring variables. The critical PRx threshold identified were 0.5 for mortality and 0.0 for favourable outcome.
Interpretation: With STARSHIP, we validate the outcome association of CA derangements as assessed by PRx in pTBI in the first prospective observational multicentre study. This provides additional evidence for the potential use of PRx for individualizing prognosis and treatment and pave way for further research in pTBI with the created database.
Funding: This study was funded by Action Medical Research for Children's Charity and Addenbrookes Charitable Trust, UK (Grant number-GN2609). Cambridge University Hospitals is the study sponsor (Reference: A094693, contact person: Michelle Ellerbeck-michelle.ellerbeck@nhs.net).
Keywords: Cerebral autoregulation; Cerebral perfusion pressure (CPP); Paediatric traumatic brain injury; Pressure reactivity index (PRx).
Crown Copyright © 2025 Published by Elsevier Ltd.
Conflict of interest statement
This research was supported by the National Institute of Health Research (NIHR) Cambridge Biomedical Research Centre (NIHR203312∗) and received support from the NIHR Clinical Research Network. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. ICM+ is a software licensed by Cambridge Enterprise Ltd. Marek Czosnyka and Peter Smielewski have a financial interest in a part of licensing fee; the licensing fee was waived for this study. Stefan Y. Bogli is supported by the Swiss National Science Foundation (grant number: 210839/225270). Claudia Smith is supported by the Patrick & Margaret Flanagan Skye Cambridge Trust Scholarship. Erta Beqiri is supported by the Medical Research Council [grant number MR N013433-1] and by the Gates Cambridge Scholarship. Peter J. Hutchinson is supported by the National Institute for Health Research (NIHR) (Senior Investigator Award, Cambridge BRC, NIHR HRC for Brain Injury) and the Royal College of Surgeons of England. None of the other authors have any further declaration of interests.
Figures


References
-
- Dewan M.C., Wellons C., III, Bonfield C.M. Epidemiology of global pediatric traumatic brain injury: qualitative review. World Neurosurg. 2016;91:497–509. - PubMed
-
- The L. The burden of traumatic brain injury in children. Lancet. 2018;391(10123):813. - PubMed
-
- Kochanek P.M., Tasker R.C., Carney N., et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the brain trauma foundation guidelines. Pediatr Crit Care Med. 2019;20(3S Suppl 1):S1–S82. - PubMed
-
- Freeman S.S., Armstead W.M., Fisk D.M., Vavilala M.S. Young age as a risk factor for impaired cerebral autoregulation after moderate to severe pediatric traumatic brian injury. Anesthesiology. 2008;108:588–595. - PubMed
LinkOut - more resources
Full Text Sources
Medical
