

Left Transradial Neurointervention Using a 3-French Simmons Guiding Sheath for a Left Carotid Approach in Patients With an Aberrant Right Subclavian Artery: A Technical Note on a Case of Preoperative Embolization of Intracranial Meningioma
- PMID: 39996182
- PMCID: PMC11848007
- DOI: 10.7759/cureus.77944
Left Transradial Neurointervention Using a 3-French Simmons Guiding Sheath for a Left Carotid Approach in Patients With an Aberrant Right Subclavian Artery: A Technical Note on a Case of Preoperative Embolization of Intracranial Meningioma
Abstract
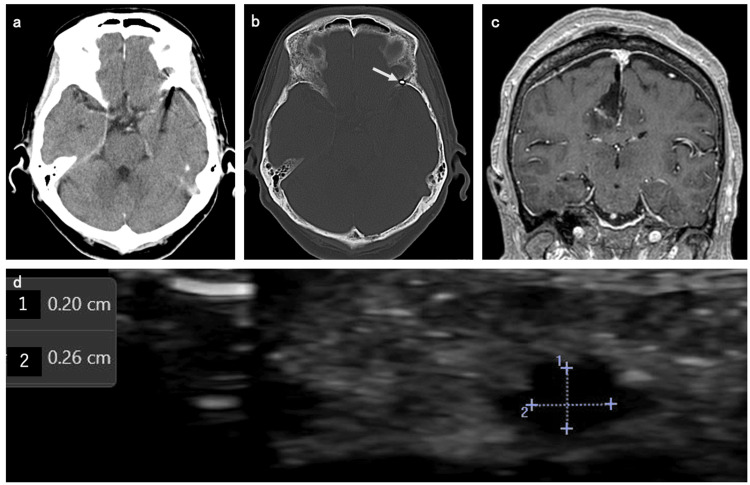
An aberrant right subclavian artery (ARSA) is a rare variant of the normal aortic arch anatomy. Right transradial carotid artery cannulation is extremely challenging in patients with ARSA. Herein, we present a case of a right falcine meningioma with an ARSA that was successfully accessed with a 3-French Simmons guiding sheath via the left transradial approach. Additionally, preoperative embolization of the feeding middle meningeal artery (MMA) was performed. Here, we report our surgical technique. An 80-year-old woman was diagnosed with a right falcine meningioma with ARSA. The meningioma exhibited tumor staining in the parietal branch of the left MMA. We planned a preoperative MMA embolization via the left radial artery. After the 3-French Simmons guiding sheath was engaged in the left common carotid artery (CCA) using the pull-back technique, a triaxial system (3-French Simmons guiding sheath/3.2-French distal access catheter/microcatheter) was implemented. The 3-French guiding sheath to the left CCA was successfully achieved using the pull-back technique. Distal access catheter guidance to the proximal left MMA was successfully achieved without catheter kinking or systemic instability. However, guiding the microcatheter beyond the pterional segment of the left MMA parietal branch because of the severe curvature and tortuosity of the vessel was difficult. Thus, embolization with liquid and particulate embolic materials was abandoned, and tumor flow reduction was performed using coil embolization of the MMA. Three days after the neurointervention, craniotomy tumor removal was successfully performed achieving near-total resection of the tumor. Thereafter, no radial artery occlusion was observed at the puncture site. The patient was discharged from our hospital two weeks after craniotomy surgery. The left transradial artery approach using a 3-French Simmons guiding sheath is useful for left carotid artery cannulation in patients with ARSA.
Keywords: arterial lusoria; left radial access; meningioma; transradial neurointervention; tumor feeding embolization.
Copyright © 2025, Sase et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



References
-
- Arteria lusoria: Developmental anatomy, clinical, radiological and surgical aspects. Myers PO, Fasel JH, Kalangos A, Gailloud P. Ann Cardiol Angeiol (Paris) 2010;59:147–154. - PubMed
-
- Aberrant right subclavian artery in fetuses with Down syndrome: A systematic review and meta-analysis. Scala C, Leone Roberti Maggiore U, Candiani M, Venturini PL, Ferrero S, Greco T, Cavoretto P. Ultrasound Obstet Gynecol. 2015;46:266–276. - PubMed
-
- Adoption of radial access and comparison of outcomes to femoral access in percutaneous coronary intervention: An updated report from the national cardiovascular data registry (2007-2012) Feldman DN, Swaminathan RV, Kaltenbach LA, et al. Circulation. 2013;127:2295–2306. - PubMed
-
- Initial experience with transradial intraoperative angiography in aneurysm clipping: Technique, feasibility, and case series. Chalouhi N, Sweid A, Al Saiegh F, et al. World Neurosurg. 2020;134:0–8. - PubMed
LinkOut - more resources
Full Text Sources