

Management of high-risk acute pulmonary embolism: an emulated target trial analysis
- PMID: 39998658
- PMCID: PMC12018524
- DOI: 10.1007/s00134-025-07805-4
Management of high-risk acute pulmonary embolism: an emulated target trial analysis
Abstract
Background: High-risk acute pulmonary embolism (PE) is a life-threatening condition necessitating hemodynamic stabilization and rapid restoration of pulmonary perfusion. In this context, evidence regarding the benefit of advanced circulatory support and pulmonary recanalization strategies is still limited.
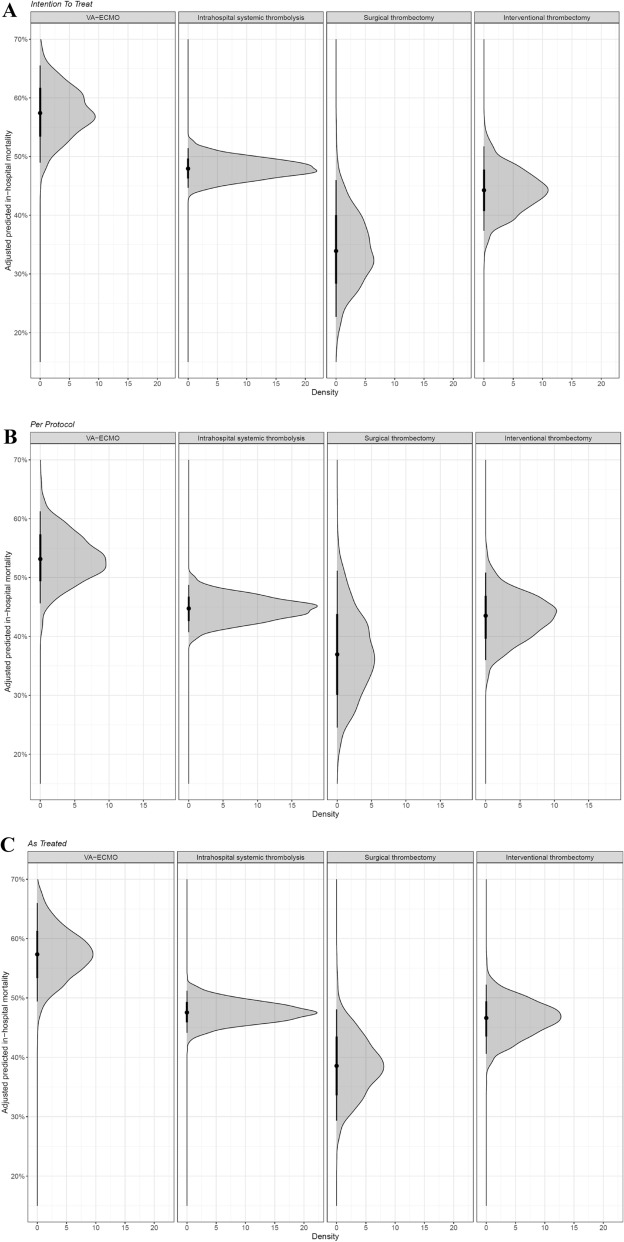
Methods: In this observational study, we assessed data of 1060 patients treated for high-risk acute PE with 991 being included in a target trial emulation to investigate all-cause in-hospital mortality estimates with different advanced treatment strategies. The four treatment groups consisted of patients undergoing (I) veno-arterial extracorporeal membrane oxygenation (VA-ECMO) alone (n = 126), (II) intrahospital systemic thrombolysis (SYS) (n = 643), (III) surgical thrombectomy (ST) (n = 49), and (IV) percutaneous catheter-directed treatment (PCDT) (n = 173). VA-ECMO was allowed as bridging to pulmonary recanalization in groups II, III, and IV. Marginal causal contrasts were estimated using the g-formula with logistic regression models as the primary approach. Sensitivity analyses included targeted maximum likelihood estimation (TMLE) with machine learning, inverse probability of treatment weighting (IPTW), as well as variations of estimands, handling of missing values, and a complete target trial emulation excluding the VA-ECMO alone group.
Results: In the overall target trial population, the median age was 62.0 years, and 53.3% of patients were male. The estimated probability of in-hospital mortality from the primary target trial intention-to-treat analysis for VA-ECMO alone was 57% (95% confidence interval [CI] 47%; 67%), compared to 48% (95% CI 44%; 53%) for intrahospital SYS, 34% (95%CI 18%; 50%) for ST, and 43% (95% CI 35%; 51%) for PCDT. The mortality risk ratios were largely in favor of any advanced recanalization strategy over VA-ECMO alone. The robustness of these findings was supported by all sensitivity analyses. In the crude outcome analysis, patients surviving to discharge had a high probability of favorable neurologic outcome in all treatment groups.
Conclusion: Advanced recanalization by means of SYS, ST, and several promising catheter-directed systems may have a positive impact on short-term survival of patients presenting with high-risk PE compared to the use of VA-ECMO alone as a bridge to recovery.
Keywords: High-risk pulmonary embolism; Mechanical circulatory support; Percutaneous catheter-directed treatment; Surgical thrombectomy; Systemic thrombolysis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: The authors declare no conflicts of interest related to this manuscript. Ethical standards: All ethical standards were met in writing and submitting this correspondence.
Figures

References
-
- Lehnert P, Lange T, Møller C et al (2018) Acute pulmonary embolism in a national Danish cohort: increasing incidence and decreasing mortality. Thromb Haemost 118:539–546. 10.1160/TH17-08-0531 - PubMed
-
- Wendelboe AM, Raskob GE (2016) Global burden of thrombosis. Circ Res 118:1340–1347. 10.1161/CIRCRESAHA.115.306841 - PubMed
-
- Centers for Disease Control and Prevention (CDC) (2012) Venous thromboembolism in adult hospitalizations - United States, 2007–2009. MMWR Morb Mortal Wkly Rep 61:401–404 - PubMed
-
- Keller K, Hobohm L, Ebner M et al (2020) Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur Heart J 41:522–529. 10.1093/eurheartj/ehz236 - PubMed
-
- Millington SJ, Aissaoui N, Bowcock E et al (2024) High and intermediate risk pulmonary embolism in the ICU. Intens Care Med 50:195–208. 10.1007/s00134-023-07275-6 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
