

Mechanical power is not associated with mortality in COVID-19 mechanically ventilated patients
- PMID: 39998751
- PMCID: PMC11861844
- DOI: 10.1186/s13613-025-01430-6
Mechanical power is not associated with mortality in COVID-19 mechanically ventilated patients
Abstract
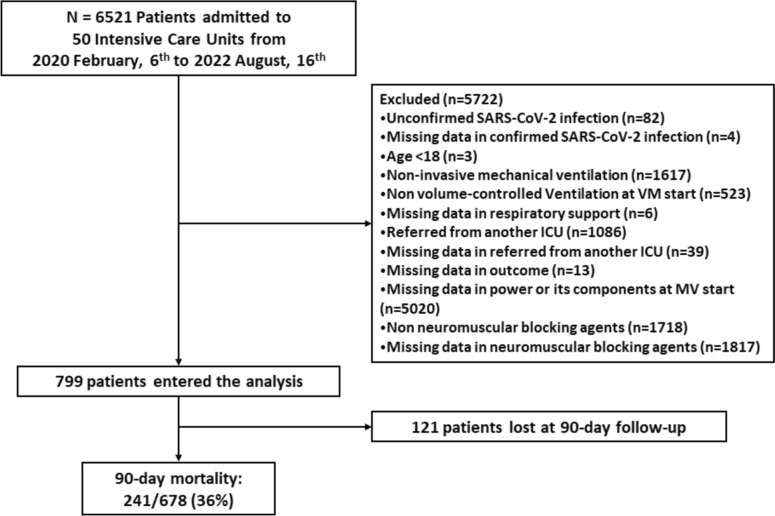
Background: The relative contribution of the different components of mechanical power to mortality is a subject of debate and has not been studied in COVID-19. The aim of this study is to evaluate both the total and the relative impact of each of the components of mechanical power on mortality in a well-characterized cohort of patients with COVID-19-induced acute respiratory failure undergoing invasive mechanical ventilation. This is a secondary analysis of the CIBERESUCICOVID project, a multicenter observational cohort study including fifty Spanish intensive care units that included COVID-19 mechanically ventilated patients between February 2020 and December 2021. We examined the association between mechanical power and its components (elastic static, elastic dynamic, total elastic and resistive power) with 90-day mortality after adjusting for confounders in seven hundred ninety-nine patients with COVID-19-induced respiratory failure undergoing invasive mechanical ventilation.
Results: At the initiation of mechanical ventilation, the PaO2/FiO2 ratio was 106 (78; 150), ventilatory ratio was 1.69 (1.40; 2.05), and respiratory system compliance was 35.7 (29.2; 44.5) ml/cmH2O. Mechanical power at the initiation of mechanical ventilation was 24.3 (18.9; 29.6) J/min, showing no significant changes after three days. In multivariable regression analyses, mechanical power and its components were not associated with 90-day mortality at the start of mechanical ventilation. After three days, total elastic and elastic static power were associated with higher 90-day mortality, but this relationship was also found for positive end-expiratory pressure.
Conclusions: Neither mechanical power nor its components were independently associated with mortality in COVID-19-induced acute respiratory failure at the start of MV. Nevertheless, after three days, static elastic power and total elastic power were associated with lower odds of survival. Positive end-expiratory pressure and plateau pressure, however, captured this risk in a similar manner.
Keywords: COVID-19; Mechanical power; Mechanical ventilation; Respiratory failure.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This is an ancillary analysis of the CIBERESUCICOVID project (NCT04457505). The study was approved by the Institution’s Internal Review Board (Comité Ètic d’Investigació Clínica, Registry number HCB/2020/0370), and informed consent was obtained from either patients or their relatives. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
References
Grants and funding
LinkOut - more resources
Full Text Sources
