

Cardiology involvement and mortality in adult patients with advanced solid cancer complicated by atrial fibrillation
- PMID: 39999078
- PMCID: PMC11856317
- DOI: 10.1371/journal.pone.0319342
Cardiology involvement and mortality in adult patients with advanced solid cancer complicated by atrial fibrillation
Abstract
Background: The association between comorbid atrial fibrillation (AF) and survival in adult patients with advanced solid cancer, as well as the impact of cardiology involvement in such patients, remains unclear.
Methods: This retrospective cohort study included adult patients diagnosed with advanced solid cancers. We calculated prevalence of AF in different cancer types and compared all-cause mortality between patients with and without AF. We further examined the association between cardiology involvement and mortality in the subset of participants with AF.
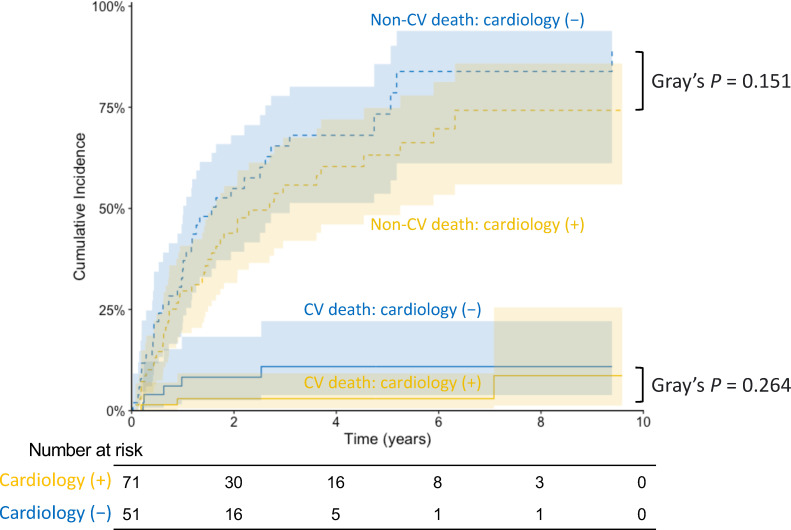
Results: Among the 1,349 adult patients with advanced solid cancer, 122 (9.0%) had AF. The risk of AF was the highest in lung and mediastinal cancer (15.6%). AF was associated with higher all-cause mortality, which became neutral after adjustment for age, sex, comorbidities, cancer types and cancer treatments (crude hazard ratio [HR] 1.39, 95% confidence interval [CI] 1.11-1.75, p = 0.004; adjusted HR 1.08, 95%CI 0.84-1.39, p = 0.552). In those with AF, cardiology involvement was independently associated with lower all-cause mortality (age, sex, comorbidities, cancer types and cancer treatments-adjusted HR 0.50 [95%CI 0.28-0.88], p = 0.017), though the cumulative incidence of neither cardiovascular nor non-cardiovascular death differed significantly between patients who received cardiology care and those who did not.
Conclusions: In adult patients with advanced solid cancer, AF per se was not independently associated with increased mortality. Cardiology involvement in patients with advanced solid cancer and AF was linked to a better overall survival, but with low certainty that this finding is not attributable to unmeasured confounding.
Copyright: © 2025 Sato et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi: 10.1093/eurheartj/ehaa612 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
