

Near-infrared fluorescence imaging with an MET-targeting probe for biopsy site selection in patients with oral potentially malignant disorders
- PMID: 39999837
- PMCID: PMC11970325
- DOI: 10.1016/j.xcrm.2025.101978
Near-infrared fluorescence imaging with an MET-targeting probe for biopsy site selection in patients with oral potentially malignant disorders
Abstract
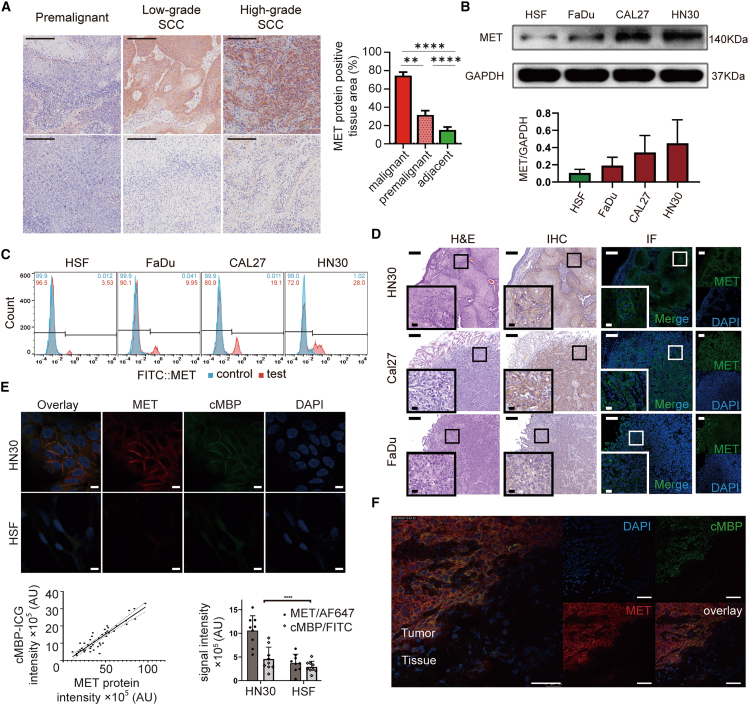
Accurate detection of malignant transformation in oral potentially malignant disorders (OPMDs) is crucial for guiding effective treatment and improving patient management. This study evaluates the potential of MET-binding peptide-indocyanine green (cMBP-ICG), a mesenchymal-epithelial transition factor (MET)-targeted near-infrared fluorescence imaging (NIRFI) probe, for biopsy site selection in OPMDs. Preclinical results demonstrate the superior accuracy of NIRFI-assisted biopsy over conventional oral examination (COE)-based biopsy in detecting high-grade dysplasia (HGD) or squamous cell carcinoma (SCC) and reducing missed detection rates. In a clinical trial with 50 patients, NIRFI-assisted biopsy achieves significantly higher diagnostic accuracy compared to COE-based biopsy (91% vs. 72%, p = 0.0005). These findings underscore the importance of NIRFI in enhancing diagnostic precision, supporting early detection and enabling timely and accurate treatment interventions for patients with OPMDs. The clinical trial is registered under the registration number ChiCTR2300074454.
Keywords: 4-NQO-induced OSCC model; biopsy site selection; fluorescence-guided biopsy; mesenchymal-epithelial transition factor; molecular imaging; near-infrared targeted fluorescent imaging; oral potentially malignant disorders; oral squamous cell carcinoma; topical application.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors have a related patent “Near-infrared fluorescence imaging agent targeting c-Met and its use” filed by X.T. et al., Shanghai Ninth People’s Hospital, China, 2022 (patent number 202210118240.6).
Figures




References
-
- Warnakulasuriya S., Kujan O., Aguirre-Urizar J.M., Bagan J.V., González-Moles M.Á., Kerr A.R., Lodi G., Mello F.W., Monteiro L., Ogden G.R., et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021;27:1862–1880. doi: 10.1111/odi.13704. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
