

Risankizumab in Japanese patients with moderate-to-severe palmoplantar pustulosis: Results from the randomized, phase 3 JumPPP study
- PMID: 40001318
- PMCID: PMC11975171
- DOI: 10.1111/1346-8138.17659
Risankizumab in Japanese patients with moderate-to-severe palmoplantar pustulosis: Results from the randomized, phase 3 JumPPP study
Abstract
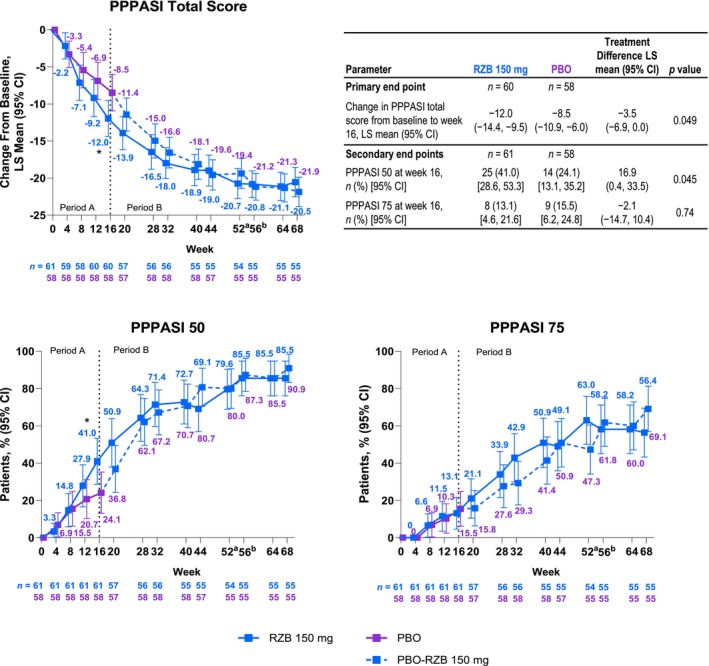
Palmoplantar pustulosis (PPP) is a chronic, debilitating skin disease of the palms and/or soles. We report the efficacy and safety of risankizumab (RZB), an interleukin 23 p19 inhibitor, from the JumPPP study (a phase 3, multicenter, randomized, placebo-controlled, double-blind study to evaluate RZB in adult Japanese sUbjects with Moderate-to-severe PalmoPlantar Pustulosis; NCT04451720). Patients were randomized 1:1 to receive RZB (150 mg) or placebo at weeks 0 and 4; all patients received RZB from week 16 to week 52 (patients initially randomized to RZB) or week 56 (patients initially randomized to placebo). The primary end point was a Palmoplantar Pustulosis Area and Severity Index (PPPASI) change from baseline; secondary end points were ≥50%/≥75% improvement in PPPASI (PPPASI 50/75) at week 16. Efficacy and safety were evaluated to 68 and 76 weeks, respectively. In total, 119 patients (RZB, n = 61; placebo, n = 58) were enrolled. Greater improvement with RZB versus placebo was demonstrated by the significant difference in PPPASI change from baseline at week 16 (least squares mean treatment difference, -3.48; p < 0.05). At week 16, a greater proportion of patients receiving RZB vs placebo achieved PPPASI 50 (41.0% vs 24.1%; nominal p < 0.05) but not PPPASI 75 (13.1% vs 15.5%; nominal p = 0.74). Improvements generally continued through to week 68. The safety profile was generally consistent with previous studies of RZB in psoriasis. RZB demonstrated efficacy over placebo at week 16 in Japanese patients with PPP, with improvements sustained through to week 68, and was well tolerated with no unexpected safety findings.
Keywords: Japan; Japanese; palmoplantar pustulosis; psoriasis; risankizumab.
© 2025 The Author(s). The Journal of Dermatology published by John Wiley & Sons Australia, Ltd on behalf of Japanese Dermatological Association.
Conflict of interest statement
Yukari Okubo has received research funds from AbbVie, Eisai, Maruho, Shiseido, Sun Pharma, and Torii. She has received honoraria for speaking, consultancy, and as an advisory board member from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Janssen, Kyowa Kirin, LEO Pharma, Maruho, Novartis, Pfizer, Sanofi, Sun Pharma, Taiho, and UCB Japan. She has received honoraria for speaking from Eisai, Jimro, Mitsubishi Tanabe, and Torii. Masamoto Murakami has received research support and/or served as a consultant for AbbVie, Amgen, Aristea Therapeutics, Boehringer Ingelheim, Bristol Myers Squibb, Eisai, Eli Lilly, Janssen, Kyowa Kirin, and Novartis. His current affiliations are with Atsuta Skin Clinic, Nagoya, Japan, and the Department of Anatomy, Histochemistry, and Cell Biology, Faculty of Medicine, University of Miyazaki, Miyazaki, Japan. Satomi Kobayashi has received research grants from Kyowa Kirin. She has received honoraria from AbbVie, Amgen, Eli Lilly, Janssen, Maruho, Novartis, and Taiho. Shigeyoshi Tsuji has received consulting fees and/or honoraria from AbbVie, Asahi Kasei Pharma, Daiichi Sankyo, Eisai, Eli Lilly, Janssen, Kyowa Kirin, Taiho, and UCB. Mitsumasa Kishimoto has received consulting fees and/or honoraria from AbbVie, Amgen, Asahi Kasei Pharma, Astellas, Ayumi Pharma, Bristol Myers Squibb, Chugai, Daiichi‐Sankyo, Eisai, Eli Lilly, Gilead, Janssen, Mitsubishi Tanabe, Novartis, Ono Pharma, Pfizer, and UCB. Kimitoshi Ikeda, Maiko Jibiki Ezequiel Neimark, Byron Padilla, and Jie Shen are full‐time employees of AbbVie Inc. or AbbVie GK, and may hold AbbVie stock or stock options. Sydney Peters is a former employee of AbbVie and may hold AbbVie stock. Tadashi Terui reports grants and/or personal fees from AbbVie, Boehringer Ingelheim, Eisai, Eli Lilly, Janssen, Kaken Pharmaceutical, Kyorin, Kyowa Kirin, Maruho, Mitsubishi Tanabe, Nihon Pharmaceutical, Novartis, Sanofi, Sun Pharma, and Taiho.
Figures



References
-
- Murakami M, Terui T. Palmoplantar pustulosis: current understanding of disease definition and pathomechanism. J Dermatol Sci. 2020;98:13–19. - PubMed
-
- Akiyama T, Seishima M, Watanabe H, Nakatani A, Mori S, Kitajima Y. The relationships of onset and exacerbation of pustulosis palmaris et plantaris to smoking and focal infections. J Dermatol. 1995;22:930–934. - PubMed
-
- Andersen YMF, Augustin M, Petersen J, Hagenström K, Mallbris L, Burge R, et al. Characteristics and prevalence of plaque psoriasis in patients with palmoplantar pustulosis. Br J Dermatol. 2019;181:976–982. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
