

doi: 10.3390/cancers17040679.
Dermoscopy of External Ear Melanocytic Lesions: Performance of Selected Dermoscopic Screening Algorithms and Proposal of a New Predictive Model for Malignancy (AuriCheck Dermoscopic Algorithm)
Affiliations
- PMID: 40002273
- PMCID: PMC11853154
- DOI: 10.3390/cancers17040679
Item in Clipboard
Dermoscopy of External Ear Melanocytic Lesions: Performance of Selected Dermoscopic Screening Algorithms and Proposal of a New Predictive Model for Malignancy (AuriCheck Dermoscopic Algorithm)
Cancers (Basel).
.
Abstract
Dermoscopy is a non-invasive imaging technique that significantly enhances diagnostic accuracy in diagnosing skin disorders [...].
Keywords: algorithm; dermoscopy; diagnostics; external ear; melanoma; nevus.
Conflict of interest statement
Luc Thomas—affiliated Institutions received dermoscopy tools and discounts for digital dermoscopy tools from HEINE Optotechnik, Casio, 3GEN, C-CUBE and FotoFinder Systems GmbH. The other authors declare no conflicts of interest.
Figures

The clinical, dermoscopic and histopathological presentation of the previously undescribed structure and pattern—‘red circles’ and ‘annular-globular pattern’. (a,b) ‘The red circles’ in nevoid melanoma. (a) The red circles are defined as the presence of continuous, complete red circles located at the periphery of the follicular openings (white arrows). (b) Round nests of atypical melanocytes with impaired maturation in depth (black ellipses) are seen in the corresponding histopathological image. Dilated perifollicular vessels are prominent (red arrows), what may correspond to the presence of ‘red circles’ observed in the dermoscopy. (c,d) The annular-globular pattern’ in Atypical Spitz Tumour. (c) The ‘annular-globular pattern’ represents globules (instead of granules) arranged concentrically around hair follicle ostia (white arrows). According to our observations, it may be characteristic for the auricular area; however, this is probably not helpful in differentiating between benign and malignant EEMLs. (d) Large diameter nests located in the interfollicular spaces (black ellipses) observed in the histopathological examination may correspond to the brown globules constituting the annular-globular pattern. Melanocytes within the nests are visible in the interfollicular spaces (hair follicles are marked with red asterisks). (a,c) FotoFinder, Medicam 800HD [FotoFinder Systems GmbH, Bad Birnbach, Germany]; 20× magnification, immersion gel. (b,d) Hematoxylin and eosin staining; magnification, 40×.

Distribution of the studied lesions across external ear anatomical sublocations. A total of 4 out of 145 (4/145; 2.8%) lesions were located within the posterior part of the auricle.

The clinical and dermoscopic spectrum of malignant EEMLs. (a) Superficial spreading melanoma (Breslow thickness 0.5 mm) of the right lobule (inset). The predominant dermoscopic structures observed on dermoscopy are regularly distributed brown globules (white arrows). The lesion is relatively symmetric in both pattern and colour and was identified as suspicious in only one of the analysed algorithms—’7-non melanoma features to rule out melanoma’. (b) Lentigo maligna of the right lobule (inset). Dermoscopy shows asymmetric pigmented follicular openings (green arrows) along with focal areas with an annular-granular pattern (red ellipse). Increased density of vascular network (black arrows) and irregular globules (white arrows) are also observed. (c) Lentigo maligna of the right scaphoid fossa (inset). Mixed pattern comprising atypical pigmented network (white arrows), parallel lines/fingerprinting (green arrow) and a brown structureless area (red arrow) is observed on dermoscopy. (d) Superficial spreading melanoma (Breslow thickness 0.3 mm) of the left helix (inset). A central area of regression manifesting as granularity/peppering (red asterisks) surrounded by a pseudonetwork (white ellipse) is visible on dermoscopy. Moreover, segmental radial lines are seen on the periphery of the lesion (black arrows). (e) Lentigo maligna melanoma (Breslow thickness 0.5 mm) of the right lobule (inset). Dermoscopy reveals the presence of a pseudonetwork (white ellipses). A small cluster of red rhomboidal structures is shown in the central bottom part of the picture (black arrow). The image was acquired in a polarized mode, and rosettes are therefore visible over red rhomboidal structures. (f) Superficial Atypical Melanocytic Proliferations of Uncertain Significance (SAMPUS) of the right lobule (inset). Dermoscopy shows an annular-granular pattern (red ellipses) associated with regression features [peppering and milky-red areas - (red asterisks)]. Focally, asymmetric pigmented follicular openings, a pseudonetwork and polygonal structures are observed (green ellipse). (a,c,d,f) FotoFinder, Medicam 800HD [FotoFinder Systems GmbH, Bad Birnbach, Germany]; 20× magnification, immersion gel. (b,e) DermLite Foto dermoscope [3Gen, San Juan Capistrano, USA] attached to a Nikon Coolpix 995 digital camera [Nikon, Tokyo, Japan]; 10× magnification, polarized light.

The clinical and dermoscopic spectrum of benign EEMLs. (a) Benign nevus of scaphoid fossa of the right ear (inset) considered benign based on over 3 years of stable clinical and videodermoscopic observation. Dermoscopy shows a typical pigmented network pattern with an eccentric area containing dotted vessels located within the ”holes” of the pigmented network (black ellipse). (b) Benign nevus of the left helix considered benign based on a stable clinical and videodermoscopic follow-up. On dermoscopy, brown structureless areas with regularly arranged globules (white arrows) are visible. (c) Spitz nevus of the left helix (inset). Dermoscopy reveals a brown structureless area, peripheral streaks (red arrows) and a centrally located pseudonetwork with ‘red circles’ (white arrows). (d) Compound nevus of the right lobule (inset). Dermoscopy shows a pseudonetwork with a centrally located small area of regression (red arrow). Adjacent to the regression area, irregular brown globules are observed (white arrows). (e) Blue nevus of the left helix (inset-black arrow). Dermoscopically, the lesion manifests with a blue-greyish structureless area with ill-defined borders. (f) Blue nevus of the right scaphoid fossa (inset). A central, structureless, white-grey-brownish area with small grey circles (black arrows) and peripheral grey-brownish hue forming a fine pseudonetwork (red arrows) is seen on dermoscopy. (a,b,c,e) FotoFinder, Medicam 800HD [FotoFinder Systems GmbH, Bad Birnbach, Germany]; 20× magnification, immersion gel. (d) DermLiteCam [3Gen, San Juan Capistrano, CA, USA]; 10× magnification, polarized light. (f) DermLite DL4 [3Gen, San Juan Capistrano, CA, USA] attached to an iPhone 11 [Apple, Cupertino, CA, USA]; 10× magnification, polarized light.
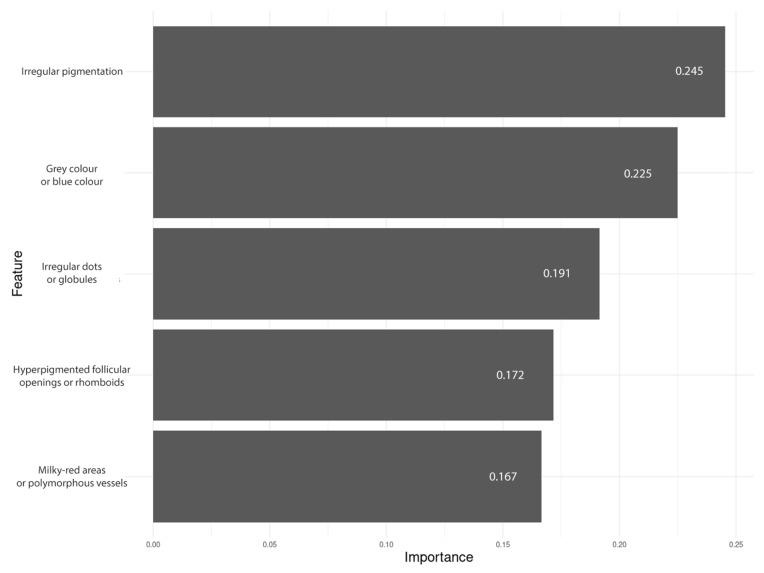
Feature importance plot of the classifier.
Similar articles
-
Clinical and Histopathologic Characteristics of Melanocytic Lesions on the Volar Skin Without Typical Dermoscopic Patterns.JAMA Dermatol. 2019 May 1;155(5):578-584. doi: 10.1001/jamadermatol.2018.5926. JAMA Dermatol. 2019. PMID: 30865233 Free PMC article.
-
Digital image analysis for diagnosis of cutaneous melanoma. Development of a highly effective computer algorithm based on analysis of 837 melanocytic lesions.Br J Dermatol. 2004 Nov;151(5):1029-38. doi: 10.1111/j.1365-2133.2004.06210.x. Br J Dermatol. 2004. PMID: 15541081 Review.
-
Modified dermoscopic algorithm for the differentiation between melanocytic and nonmelanocytic skin tumors.J Cutan Med Surg. 2006 Mar-Apr;10(2):73-8. doi: 10.2310/7750.2006.00021. J Cutan Med Surg. 2006. PMID: 17241578
-
Reliability and inter-observer agreement of dermoscopic diagnosis of melanoma and melanocytic naevi. Dermoscopy Panel.Eur J Cancer Prev. 1998 Oct;7(5):397-402. doi: 10.1097/00008469-199810000-00005. Eur J Cancer Prev. 1998. PMID: 9884886
-
[Basic dermoscopy of melanocytic lesions for beginners].Postepy Hig Med Dosw (Online). 2011 Aug 8;65:501-8. doi: 10.5604/17322693.955121. Postepy Hig Med Dosw (Online). 2011. PMID: 21918252 Review. Polish.
References
-
- Longo C., Pampena R., Moscarella E., Chester J., Starace M., Cinotti E., Piraccini B.M., Argenziano G., Peris K., Pellacani G. Dermoscopy of melanoma according to different body sites: Head and neck, trunk, limbs, nail, mucosal and acral. J. Eur. Acad. Dermatol. Venereol. 2023;37:1718–1730. doi: 10.1111/jdv.19221. - DOI - PubMed
-
- Micantonio T., Neri L., Longo C., Grassi S., Di Stefani A., Antonini A., Coco V., Fargnoli M.C., Argenziano G., Peris K. A new dermoscopic algorithm for the differential diagnosis of facial lentigo maligna and pigmented actinic keratosis. Eur. J. Dermatol. 2018;28:162–168. doi: 10.1684/ejd.2018.3246. - DOI - PubMed
LinkOut - more resources
Full Text Sources
