

Bladder Endometriosis: Diagnostic, Therapy, and Outcome of a Single-Center Experience
- PMID: 40002617
- PMCID: PMC11854327
- DOI: 10.3390/diagnostics15040466
Bladder Endometriosis: Diagnostic, Therapy, and Outcome of a Single-Center Experience
Abstract
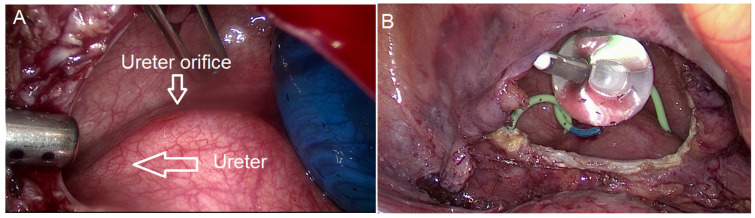
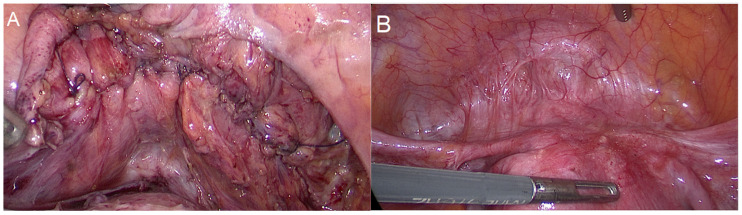
Background/Objectives: Endometriosis is a benign condition affecting up to 10% of women at reproductive age. The urinary tract is affected in 0.3-12.0% of women with endometriosis and in 19.0-53.0% of women with deep infiltrating endometriosis. The bladder is the most commonly affected organ in the urinary tract. Bladder endometriosis is defined by the presence of endometriosis lesions in the detrusor muscle, with partial or complete thickness involvement. Methods: This was a retrospective study. The study analyzed surgical reports of 11,714 patients who underwent endometriosis laparoscopy, and included only 42 patients with bladder endometriosis. Results: We found that 0.35% of patients with endometriosis had bladder endometriosis. In total, 29 patients underwent phone follow-up. In total, 26 patients (90%) reported a general improvement in their symptoms (e.g., improving the dysmenorrhea, lower abdominal pain), with a 100% improvement in their dysuria. Only two patients (7%) reported no change in symptoms (dysmenorrhea and dyspareunia). Conclusions: Gynecologists can perform laparoscopic surgical treatment of bladder endometriosis in most cases. If ureteroneocystostomy is required or the localization of the endometriosis nodule is unfavorable, an intervention by an interdisciplinary team is recommended. Both laparoscopic partial bladder resection and shaving can be considered effective methods with low complication risk. This surgical approach requires excellent laparoscopic skills.
Keywords: DIE; bladder endometriosis; bladder shaving; dysuria; hematuria; laparoscopy; partial bladder resection.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Laparoscopic Approach in Bladder Endometriosis, Intraoperative and Postoperative Outcomes.In Vivo. 2023 Jan-Feb;37(1):357-365. doi: 10.21873/invivo.13086. In Vivo. 2023. PMID: 36593051 Free PMC article.
-
Endometriosis of bladder: outcomes after laparoscopic surgery.J Minim Invasive Gynecol. 2010 Sep-Oct;17(5):600-4. doi: 10.1016/j.jmig.2010.05.008. Epub 2010 Jul 24. J Minim Invasive Gynecol. 2010. PMID: 20656568
-
Bladder Endometriosis: Management by Cystoscopic and Laparoscopic Approaches.J Minim Invasive Gynecol. 2019 Jul-Aug;26(5):807-808. doi: 10.1016/j.jmig.2018.09.782. Epub 2018 Sep 29. J Minim Invasive Gynecol. 2019. PMID: 30278234
-
Laparoscopic surgery with urinary tract reconstruction and bowel endometriosis resection for deep infiltrating endometriosis.Asian J Endosc Surg. 2018 Feb;11(1):7-14. doi: 10.1111/ases.12464. Epub 2018 Feb 14. Asian J Endosc Surg. 2018. PMID: 29444547 Review.
-
A Combined Approach: Laparoscopic Partial Bladder Prior Transurethral Resection for Bladder Endometriosis-Case Report and Surgical Video Presentation.Urology. 2023 Aug;178:187-189. doi: 10.1016/j.urology.2023.05.011. Epub 2023 May 23. Urology. 2023. PMID: 37230270 Review.
Cited by
-
Is there a relationship between symptoms and types of endometriosis according to #ENZIAN? A comparative study of preoperative questionnaires.Arch Gynecol Obstet. 2025 Sep;312(3):969-977. doi: 10.1007/s00404-025-08072-w. Epub 2025 Jun 28. Arch Gynecol Obstet. 2025. PMID: 40580252 Free PMC article.
-
Does BMI Have an Impact on Endometriosis Symptoms and Endometriosis Types According to the #ENZIAN Classification?J Clin Med. 2025 Jun 7;14(12):4040. doi: 10.3390/jcm14124040. J Clin Med. 2025. PMID: 40565786 Free PMC article.
References
-
- International Working Group of AAGL, ESGE, ESHRE and WES. Tomassetti C., Johnson N.P., Petrozza J., Abrao M.S., Einarsson J.I., Horne A.W., Lee T.T.M., Missmer S., Vermeulen N., et al. An International Terminology for Endometriosis, 2021. J. Minim. Invasive Gynecol. 2021;28:1849–1859. doi: 10.1016/j.jmig.2021.08.032. - DOI - PubMed
LinkOut - more resources
Full Text Sources
