

Cryoballoon Pulmonary Vein Isolation in Obese Patients with Atrial Fibrillation Compared to Non-Obese Counterparts: A Meta-Analysis
- PMID: 40002711
- PMCID: PMC11852532
- DOI: 10.3390/biomedicines13020298
Cryoballoon Pulmonary Vein Isolation in Obese Patients with Atrial Fibrillation Compared to Non-Obese Counterparts: A Meta-Analysis
Abstract
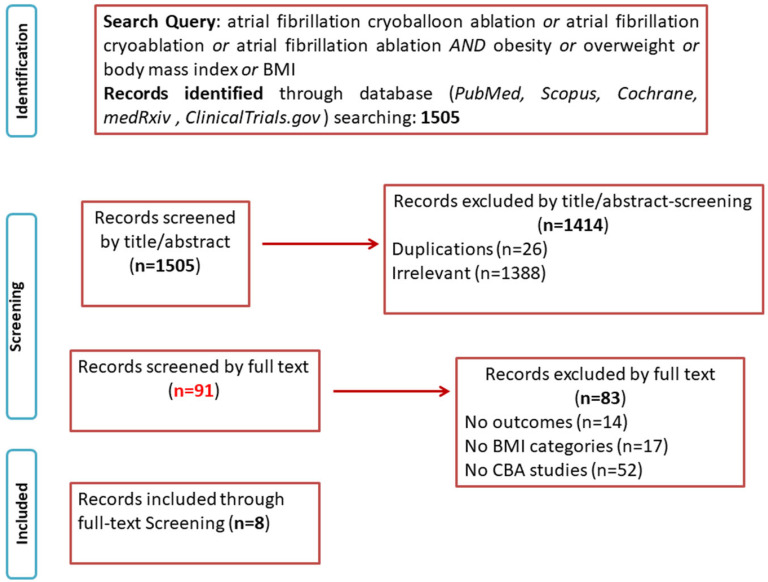
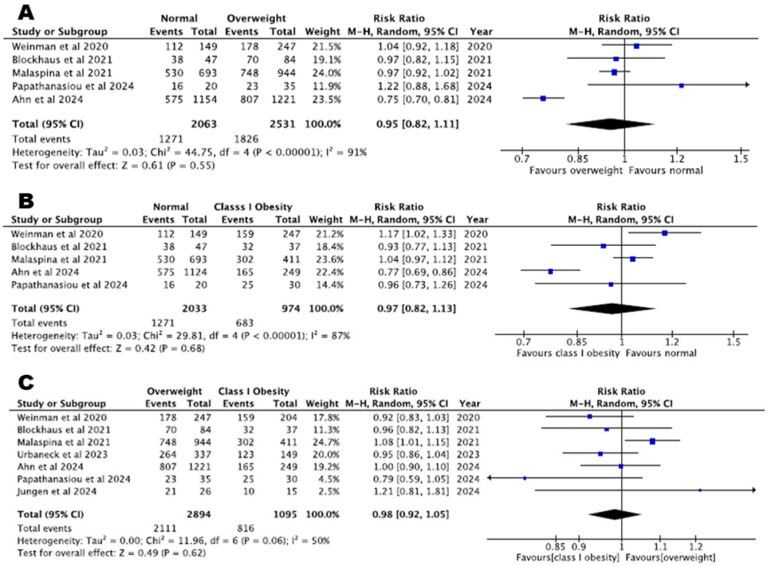
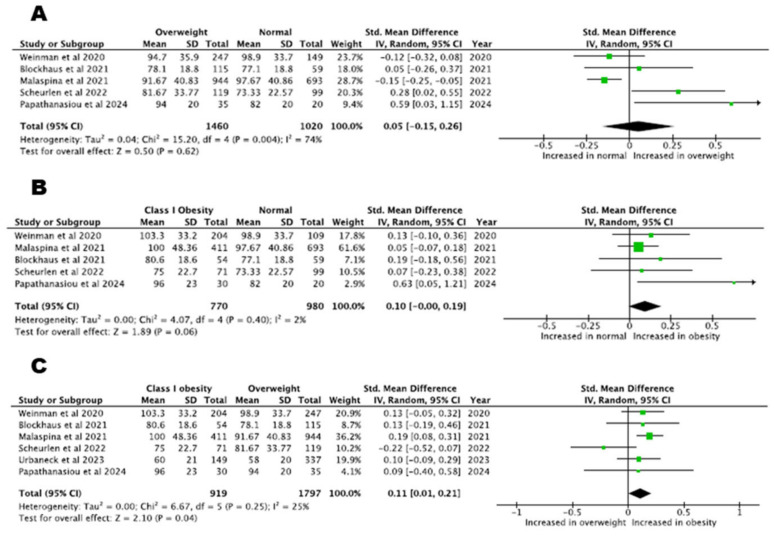
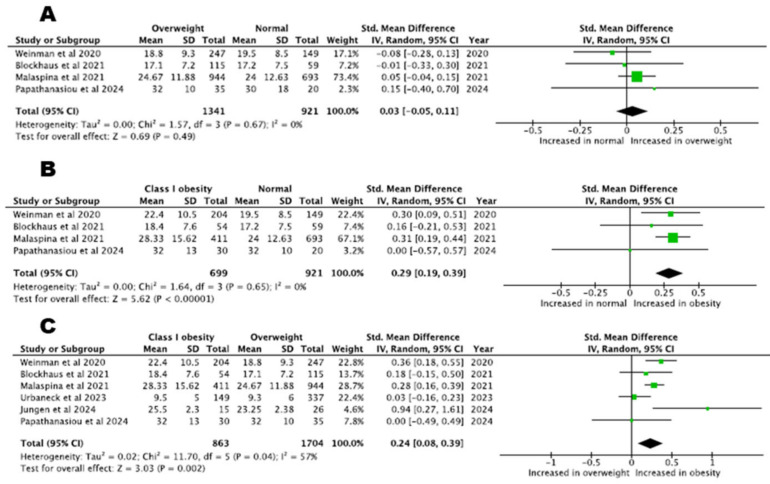
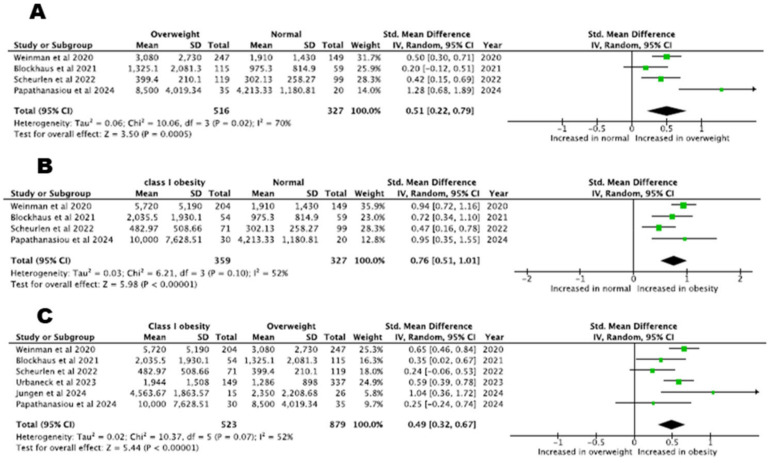
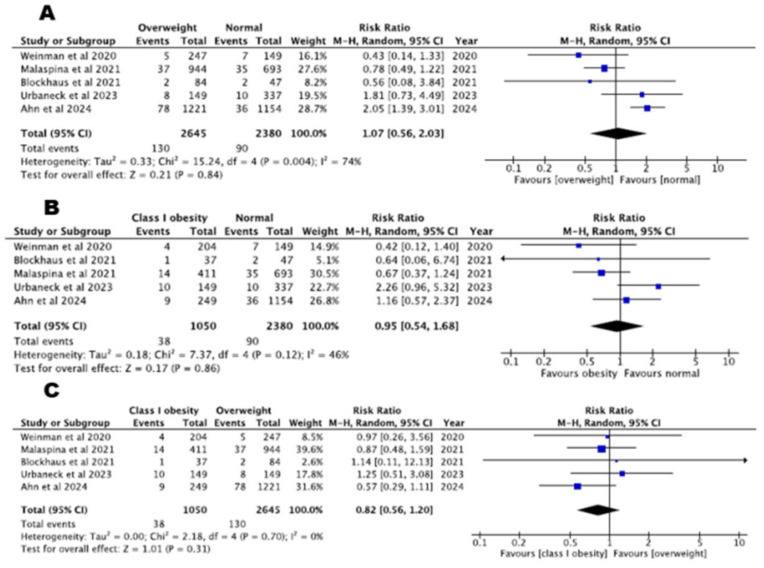
Introduction: Obesity is an important risk factor for atrial fibrillation (AF) development. Data on cryoballoon ablation (CBA) outcomes in obese patients have so far been scarce. We reviewed the existing literature to compare the efficacy and safety of CBA in obese versus non-obese AF patients. Methods: A systematic literature search was conducted for studies comparing clinical outcomes (arrhythmia recurrence and/or procedural data and/or safety outcomes) between obese and non-obese patients undergoing CBA for AF. Statistical pooling was performed according to a random-effects model with generic inverse-variance weighting of relative risks (RRs) and standardised mean differences (SMDs) computing risk estimates with 95% confidence intervals (CIs). Results: Obese and non-obese patients had comparable arrhythmia recurrence rates (normal versus overweight, RR = 0.95, 95% CI: 0.82-1.11, p = 0.55, I2% = 91%; normal versus class I obesity, RR = 0.97, 95% CI: 0.82-1.13, p = 0.68, I2% = 87%; normal versus class II obesity, RR = 0.98, 95% CI: 0.91-1.07, p = 0.29, I2% = 65%). Procedure time was marginally increased in obese patients compared to non-obese counterparts (normal versus overweight, SMD = 0.05, 95% CI: -0.15-0.26, p = 0.62, I2% = 74%; normal versus class I obesity, SMD = 0.10, 95% CI: -0.00-0.19, p = 0.06, I2% = 2%; overweight versus class I obesity, SMD = 0.11, 95% CI: 0.01-0.21, p = 0.048, I2% = 25%). Regarding radiation exposure, fluoroscopy time was increased in patients with class I obesity compared to normal-weight or overweight patients and dose area product was also increased in obese patients compared to non-obese patients. Lastly, the risk of complications did not differ between obese and non-obese patients. Statistical heterogeneity and the small number of patients included are the main limitations of this study. Conclusion: CBA seems to be effective for obese patients suffering from AF, featuring also similar safety outcomes with non-obese individuals. Radiation exposure was increased in obese patients.
Keywords: arrhythmia recurrence; atrial fibrillation; body mass index; catheter ablation; obesity; radiation exposure.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Pulmonary vein isolation with the cryoballoon in obese atrial fibrillation patients - Does weight have an impact on procedural parameters and clinical outcome?Int J Cardiol. 2020 Oct 1;316:137-142. doi: 10.1016/j.ijcard.2020.06.001. Epub 2020 Jun 6. Int J Cardiol. 2020. PMID: 32522675
-
Impact of Body Mass Index on the Outcomes of Cryoballoon Pulmonary Vein Isolation for Paroxysmal Atrial Fibrillation.Clin Pract. 2024 Nov 12;14(6):2463-2474. doi: 10.3390/clinpract14060192. Clin Pract. 2024. PMID: 39585020 Free PMC article.
-
Increased rates of atrial fibrillation recurrence following pulmonary vein isolation in overweight and obese patients.J Cardiovasc Electrophysiol. 2018 Feb;29(2):239-245. doi: 10.1111/jce.13388. Epub 2017 Dec 14. J Cardiovasc Electrophysiol. 2018. PMID: 29131442
-
A systematic review and meta-analysis comparing second-generation cryoballoon and contact force radiofrequency ablation for initial ablation of paroxysmal and persistent atrial fibrillation.J Cardiovasc Electrophysiol. 2020 Oct;31(10):2559-2571. doi: 10.1111/jce.14676. Epub 2020 Jul 23. J Cardiovasc Electrophysiol. 2020. PMID: 32671920
-
Comparative safety and effectiveness of cryoballoon versus radiofrequency ablation for atrial fibrillation: a systematic review and meta-analysis.Egypt Heart J. 2025 Feb 3;77(1):18. doi: 10.1186/s43044-025-00611-9. Egypt Heart J. 2025. PMID: 39899186 Free PMC article. Review.
Cited by
-
Safety and efficacy of high- and very high-power short-duration ablation in overweight and obese patients with atrial fibrillation.Heart Vessels. 2025 May 27. doi: 10.1007/s00380-025-02560-4. Online ahead of print. Heart Vessels. 2025. PMID: 40423792
References
-
- Chatterjee N.A., Giulianini F., Geelhoed B., Lunetta K.L., Misialek J.R., Niemeijer M.N., Rienstra M., Rose L.M., Smith A.V., Arking D.E., et al. Genetic Obesity and the Risk of Atrial Fibrillation: Causal Estimates from Mendelian Randomization. Circulation. 2017;135:741–754. doi: 10.1161/CIRCULATIONAHA.116.024921. - DOI - PMC - PubMed
-
- Wong C.X., Sullivan T., Sun M.T., Mahajan R., Pathak R.K., Middeldorp M., Twomey D., Ganesan A.N., Rangnekar G., Roberts-Thomson K.C., et al. Obesity and the Risk of Incident, Post-Operative, and Post-Ablation Atrial Fibrillation: A Meta-Analysis of 626,603 Individuals in 51 Studies. JACC. Clin. Electrophysiol. 2015;1:139–152. doi: 10.1016/j.jacep.2015.04.004. - DOI - PubMed
-
- Aune D., Sen A., Schlesinger S., Norat T., Janszky I., Romundstad P., Tonstad S., Riboli E., Vatten L.J. Body mass index, abdominal fatness, fat mass and the risk of atrial fibrillation: A systematic review and dose–response meta-analysis of prospective studies. Eur. J. Epidemiol. 2017;32:181–192. doi: 10.1007/s10654-017-0232-4. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
