

Anatomy-Based Filler Injection: Treatment Techniques for Supraorbital Hollowness and Charming Roll
- PMID: 40003713
- PMCID: PMC11857838
- DOI: 10.3390/life15020304
Anatomy-Based Filler Injection: Treatment Techniques for Supraorbital Hollowness and Charming Roll
Abstract
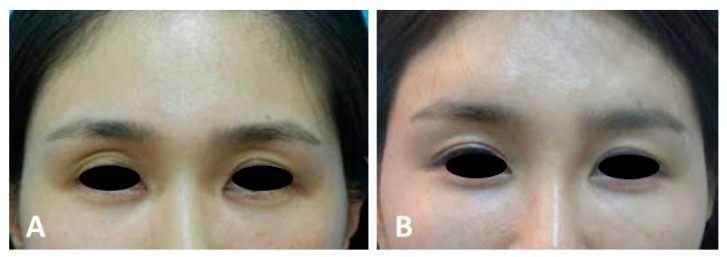
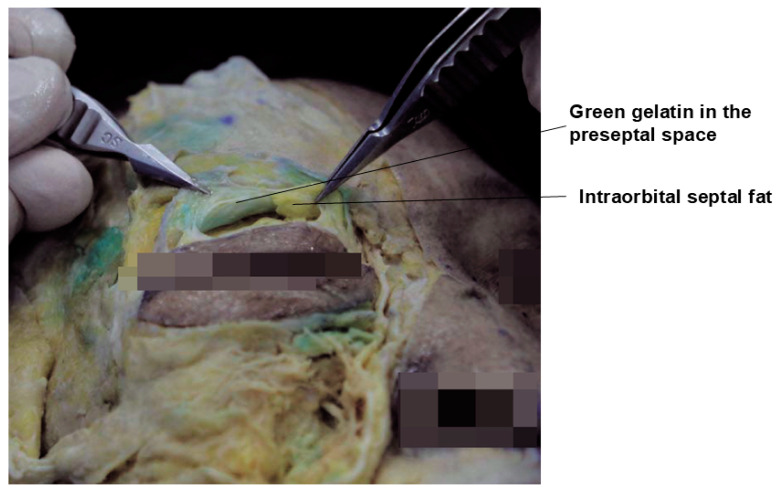
Supraorbital hollowness and pretarsal fullness, commonly known as the sunken eyelid and charming roll, respectively, are significant anatomical features that impact the aesthetic appearance of the periorbital region. Supraorbital hollowness is characterized by a recessed appearance of the upper eyelid, often attributed to genetic factors, aging, or surgical alterations, such as excessive fat removal during blepharoplasty. This condition is particularly prevalent among East Asians due to anatomical differences, such as weaker levator muscles and unique fat distribution patterns. Pretarsal fullness, also known as aegyo-sal, enhances the youthful and expressive appearance of the lower eyelid, forming a roll above the lash line that is considered aesthetically desirable in East Asian culture. Anatomical-based filler injection techniques are critical for correcting these features, involving precise placement within the correct tissue planes to avoid complications and achieve natural-looking results. This approach not only improves the aesthetic appeal of the eyelid but also enhances the overall facial harmony, emphasizing the importance of tailored procedures based on individual anatomy and cultural preferences.
Keywords: eyebrow anatomy; hyaluronic acid fillers; periorbital rejuvenation; pretarsal fullness; supraorbital hollowness.
Conflict of interest statement
Author Jovian Wan was employed by the Medical Research Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures













References
-
- Wakade D.V., Nayak C.S., Bhatt K.D. A Study Comparing the Efficacy of Monopolar Radiofrequency and Glycolic Acid Peels in Facial Rejuvenation of Aging Skin Using Histopathology and Ultrabiomicroscopic Sonography (UBM)—An Evidence Based Study. Acta Medica. 2016;59:14–17. doi: 10.14712/18059694.2016.49. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
