

Autoimmune Pancreatitis Mimicking a Pancreatic Neuroendocrine Tumor: A Case Report with a Literature Review
- PMID: 40004001
- PMCID: PMC11855540
- DOI: 10.3390/ijms26041536
Autoimmune Pancreatitis Mimicking a Pancreatic Neuroendocrine Tumor: A Case Report with a Literature Review
Abstract
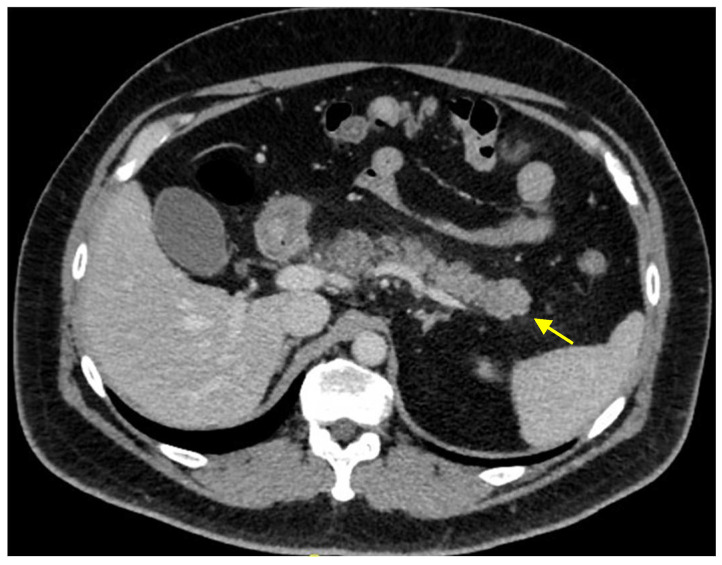
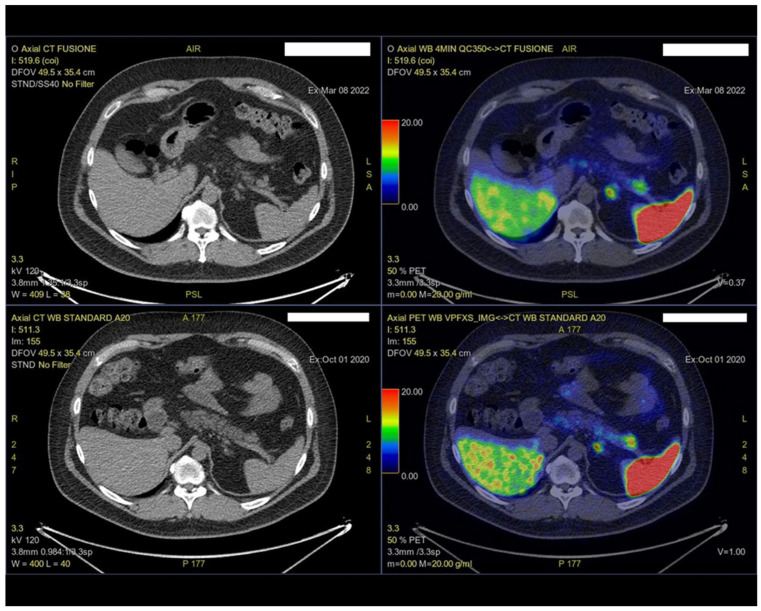
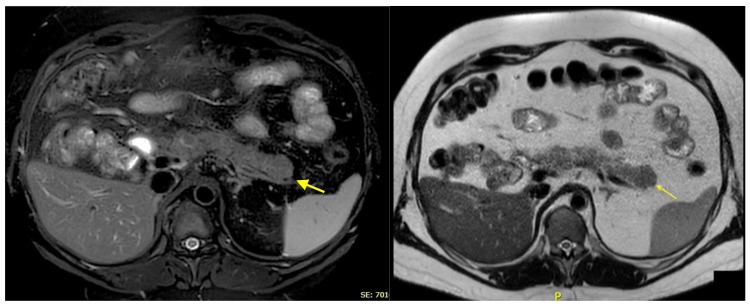
Autoimmune pancreatitis (AIP) is a rare chronic pancreatitis subtype that often mimics pancreatic cancer due to the overlapping clinical and radiological features, posing significant diagnostic challenges. Similarly, distinguishing AIP from pancreatic neuroendocrine neoplasms (PanNENs), which present with nonspecific symptoms, adds complexity to clinical evaluations. We present the case of a 46-year-old male with recurrent acute idiopathic pancreatitis. Abdominal computed tomography (CT) revealed a 25 mm hypodense mass in the pancreatic tail with mild arterial contrast enhancement. Magnetic resonance imaging (MRI) showed the mass to be hypointense on T2-weighted sequences, with no diffusion restriction and an enhancement pattern akin to normal pancreatic tissue. The endoscopic ultrasound-guided fine needle biopsy (EUS-FNB) was inconclusive. Gallium-68 DOTATATE positron emission tomography-CT (Ga-68 DOTATATE PET-CT) showed an increased tracer uptake, leading to a distal pancreatectomy with a splenectomy. Histopathology demonstrated chronic sclerotic pancreatitis with inflammatory infiltrates. Elevated serum IgG4 levels confirmed the diagnosis of type 1 AIP Differentiating AIP from pancreatic malignancies, including PanNENs, is both critical and complex. This case highlights a misdiagnosis of PanNENs in a patient with focal AIP, where neuroendocrine hyperplasia and islet cell clusters within fibrotic areas mimicked PanNENs, even on Ga-68 PET-CT. The findings emphasize the potential for false positives with Ga-68 DOTATATE PET-CT and the importance of integrating clinical, radiological, and histological data for an accurate diagnosis.
Keywords: autoimmune pancreatitis; chronic pancreatitis; pancreatic neuroendocrine tumors.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Focal Pancreatitis Mimicking Neuroendocrine Tumor on DOTATATE PET/CT With Radiology-Pathology Correlation.Clin Nucl Med. 2024 Dec 1;49(12):1124-1125. doi: 10.1097/RLU.0000000000005516. Epub 2024 Oct 10. Clin Nucl Med. 2024. PMID: 39385385
-
Pancreatic tumor in type 1 autoimmune pancreatitis: a diagnostic challenge.BMC Cancer. 2019 Aug 16;19(1):814. doi: 10.1186/s12885-019-6027-0. BMC Cancer. 2019. PMID: 31419961 Free PMC article.
-
Concomitant Pancreatic Ductal Adenocarcinoma and Type 1 Autoimmune Pancreatitis: A Potential Issue in the Diagnosis of Carcinoma by Endoscopic Ultrasound-guided Fine-needle Biopsy.Intern Med. 2023 Feb 15;62(4):545-551. doi: 10.2169/internalmedicine.0075-22. Epub 2022 Jul 14. Intern Med. 2023. PMID: 35831103 Free PMC article.
-
Localized Autoimmune Pancreatitis: Report of a Case Clinically Mimicking Pancreatic Cancer and a Literature Review.Medicine (Baltimore). 2015 Oct;94(42):e1656. doi: 10.1097/MD.0000000000001656. Medicine (Baltimore). 2015. PMID: 26496272 Free PMC article. Review.
-
Focal Autoimmune Pancreatitis Morphologically Mimicking Pancreatic Cancer: A Case Report and Literature Review.Am J Case Rep. 2024 Sep 16;25:e944286. doi: 10.12659/AJCR.944286. Am J Case Rep. 2024. PMID: 39279197 Free PMC article. Review.
References
-
- Shimosegawa T., Chari S.T., Frulloni L., Kamisawa T., Kawa S., Mino-Kenudson M., Kim M.H., Klöppel G., Lerch M.M., Löhr M., et al. International consensus diagnostic criteria for autoimmune pancreatitis: Guidelines of the International Association of Pancreatology. Pancreas. 2011;40:352–358. doi: 10.1097/MPA.0b013e3182142fd2. - DOI - PubMed
-
- Löhr J.M., Beuers U., Vujasinovic M., Alvaro D., Frøkjær J.B., Buttgereit F., Capurso G., Culver E.L., de-Madaria E., Della-Torre E., et al. European Guideline on IgG4-related digestive disease—UEG and SGF evidence-based recommendations. United Eur. Gastroenterol. J. 2020;8:637–666. doi: 10.1177/2050640620934911. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
