

Spinal Cord Infarction: Clinical and Neuroradiological Clues of a Rare Stroke Subtype
- PMID: 40004823
- PMCID: PMC11856212
- DOI: 10.3390/jcm14041293
Spinal Cord Infarction: Clinical and Neuroradiological Clues of a Rare Stroke Subtype
Abstract
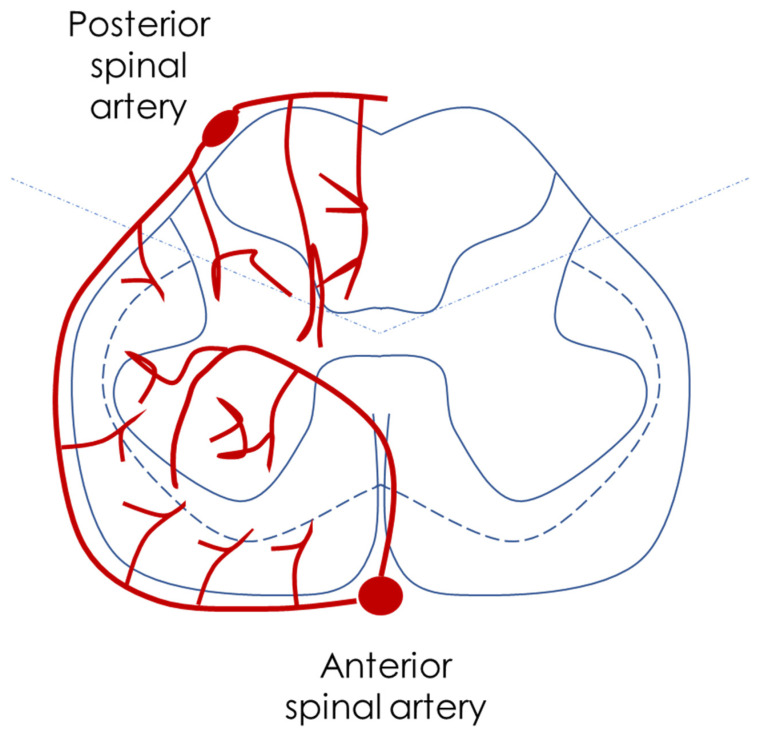
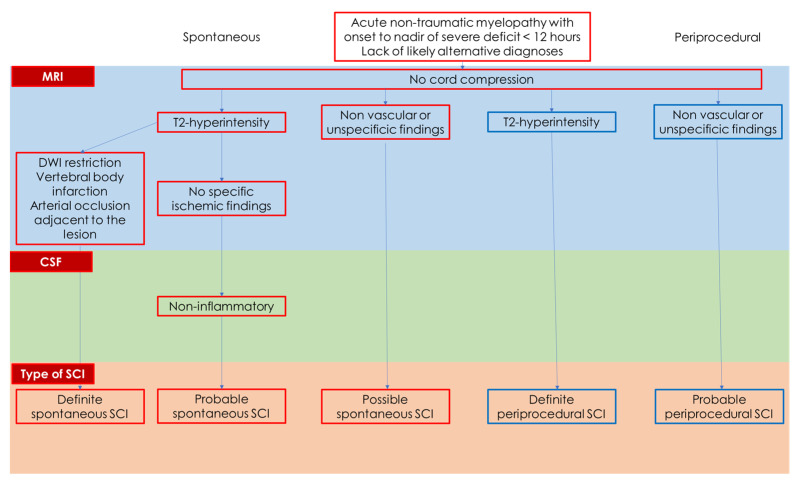
Spinal cord infarction (SCI) of arterial origin is a rare vascular event, and its incidence is probably underestimated. There are no strong epidemiological data, and the diagnostic pathway is complex and sometimes incomplete. Furthermore, many cases may be misdiagnosed as other forms of acute and subacute myelopathies. The focus of this review is the clinical and neuroradiological issues in diagnosing SCI and their respective reliability in a clinical setting. The new proposed diagnostic criteria of SCI, although not covering all aspects, highlight the need for a comprehensive approach, including even atypical cases, as the lack of cord compression on Magnetic Resonance Imaging (MRI) is the only mandatory feature for diagnosis. Some MRI features are supportive of the diagnosis, particularly when the anterior spinal artery territory is involved and diffusion-weighted imaging (DWI) is used. Several etiologies can be considered, considering traditional vascular risk factors and diseases affecting the aorta and its main branches, yet a significant proportion of cases remain without a definite etiology. The strongest predictor of SCI diagnosis is a clinical variable, i.e., a time to nadir of severe deficits < 12 h.
Keywords: DWI; MRI; aorta; dissection; owl’s eyes; periprocedural; spinal cord infarction; time.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






Similar articles
-
The utility of diffusion-weighted imaging in patients with spinal cord infarction: difference from the findings of neuromyelitis optica spectrum disorder.BMC Neurol. 2022 Oct 11;22(1):382. doi: 10.1186/s12883-022-02903-y. BMC Neurol. 2022. PMID: 36221057 Free PMC article.
-
Characteristics of Spontaneous Spinal Cord Infarction and Proposed Diagnostic Criteria.JAMA Neurol. 2019 Jan 1;76(1):56-63. doi: 10.1001/jamaneurol.2018.2734. JAMA Neurol. 2019. PMID: 30264146 Free PMC article.
-
Clinical manifestations and magnetic resonance imaging features of spinal cord infarction.J Neuroradiol. 2024 Jun;51(4):101158. doi: 10.1016/j.neurad.2023.10.003. Epub 2023 Oct 8. J Neuroradiol. 2024. PMID: 37816441
-
Hyperacute extensive spinal cord infarction and negative spine magnetic resonance imaging: a case report and review of the literature.Medicine (Baltimore). 2020 Oct 23;99(43):e22900. doi: 10.1097/MD.0000000000022900. Medicine (Baltimore). 2020. PMID: 33120840 Free PMC article. Review.
-
Spinal cord infarction: A systematic review and meta-analysis of patient's characteristics, diagnosis accuracy, management, and outcome.Surg Neurol Int. 2024 Sep 13;15:325. doi: 10.25259/SNI_477_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39372971 Free PMC article. Review.
Cited by
-
Spinal cord infarction following neurointerventional procedures in the posterior cerebral circulation: a case analysis and systematic literature review.BMC Neurol. 2025 May 29;25(1):232. doi: 10.1186/s12883-025-04255-9. BMC Neurol. 2025. PMID: 40442615 Free PMC article. Review.
References
-
- [(accessed on 7 November 2024)]. Available online: https://icd.who.int/en.
-
- Sacco R.L., Kasner S.E., Broderick J.P., Caplan L.R., Connors J.J., Culebras A., Elkind M.S., George M.G., Hamdan A.D., Higashida R.T., et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44:2064–2089. doi: 10.1161/STR.0b013e318296aeca. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
