

Should the Right Coronary Artery Be Routinely Assessed During Provocative Spasm Testing?
- PMID: 40004885
- PMCID: PMC11856602
- DOI: 10.3390/jcm14041355
Should the Right Coronary Artery Be Routinely Assessed During Provocative Spasm Testing?
Abstract
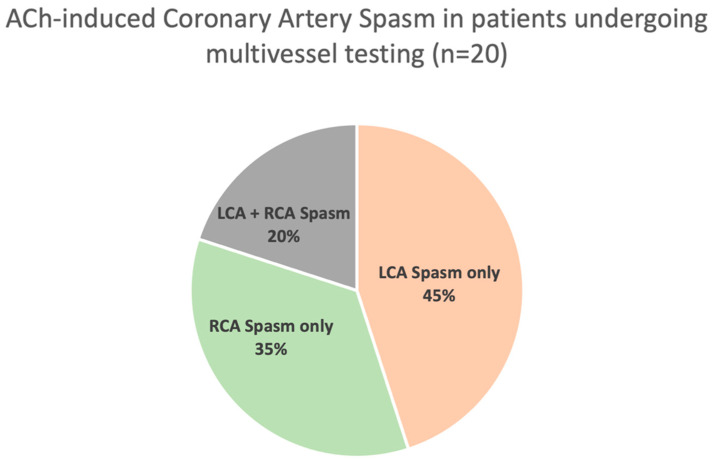
Background/Objectives: The diagnosis of coronary artery spasm (CAS) frequently requires invasive provocation testing, typically utilising acetylcholine (ACh). Although the left coronary artery (LCA) is routinely assessed as a part of the testing protocol, assessment of the right coronary artery (RCA) is often avoided since it requires the insertion of a temporary pacing wire. We sought to compare the prevalence of inducible CAS in the LCA and RCA, among patients with CAS undergoing multivessel spasm provocation testing with ACh. Methods: A local multi-institutional ANOCA (angina and non-obstructive coronary arteries) database was analysed, which included 316 patients with angina and suspected CAS who underwent provocation testing (single vessel n = 266, multivessel n = 50) with incremental bolus doses of intracoronary ACh (25, 50, 100 μg in the LCA; 25, 50 μg in the RCA). CAS was defined as >90% constriction of the epicardial coronary artery as assessed visually on coronary angiography. Results: In the 50 patients (55 ± 10 years, 77% female) who underwent multivessel spasm provocation testing, CAS was induced in 20 patients (40%), with ACh provoking CAS only in the LCA system in 45%, only in the RCA system in 35%, and both LCA/RCA in 20%. Conclusions: These findings demonstrate that assessing only the LCA may miss up to one-third of CAS cases. Therefore, it is essential to routinely evaluate the RCA, particularly when no inducible spasm is detected in the LCA.
Keywords: ANOCA; angina with non-obstructive coronary arteries; coronary artery spasm; functional coronary angiography; multivessel testing; provocative spasm testing.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Jespersen L., Hvelplund A., Abildstrøm S.Z., Pedersen F., Galatius S., Madsen J.K., Jørgensen E., Kelbæk H., Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur. Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331. - DOI - PubMed
-
- Samuels B.A., Shah S.M., Widmer R.J., Kobayashi Y., Miner S.E.S., Taqueti V.R., Jeremias A., Albadri A., Blair J.A., Kearney K.E., et al. Comprehensive Management of ANOCA, Part 1—Definition, Patient Population, and Diagnosis. J. Am. Coll. Cardiol. 2023;82:1245–1263. doi: 10.1016/j.jacc.2023.06.043. - DOI - PubMed
-
- Smilowitz N.R., Prasad M., Widmer R.J., Toleva O., Quesada O., Sutton N.R., Lerman A., Reynolds H.R., Kesarwani M., Savage M.P., et al. Comprehensive Management of ANOCA, Part 2—Program Development, Treatment, and Research Initiatives. J. Am. Coll. Cardiol. 2023;82:1264–1279. doi: 10.1016/j.jacc.2023.06.044. - DOI - PubMed
-
- Konst R.E., Damman P., Pellegrini D., Hartzema-Meijer M.J., van Uden B.J.C., Jansen T.P.J., Brandsma J., Vart P., Gehlmann H., Maas A., et al. Vasomotor dysfunction in patients with angina and nonobstructive coronary artery disease is dominated by vasospasm. Int. J. Cardiol. 2021;333:14–20. doi: 10.1016/j.ijcard.2021.02.079. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
