

Urinary Dopamine Levels Can Predict the Avidity of Post-Therapy [131I]MIBG Scintigraphy in Unresectable or Metastatic Pheochromocytomas and Paragangliomas: A Preliminary Clinical Study
- PMID: 40005979
- PMCID: PMC11858449
- DOI: 10.3390/ph18020165
Urinary Dopamine Levels Can Predict the Avidity of Post-Therapy [131I]MIBG Scintigraphy in Unresectable or Metastatic Pheochromocytomas and Paragangliomas: A Preliminary Clinical Study
Abstract
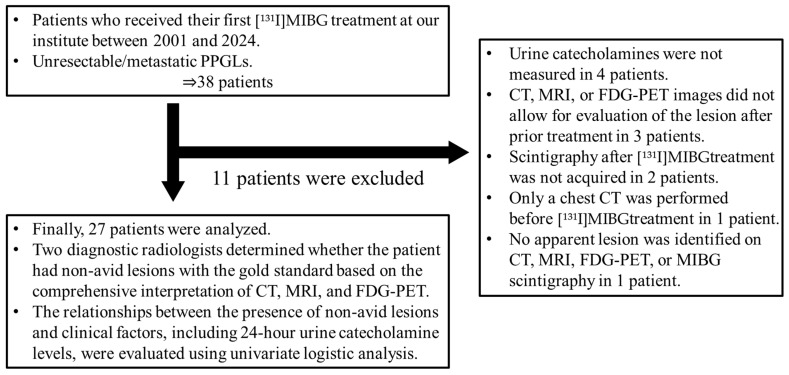
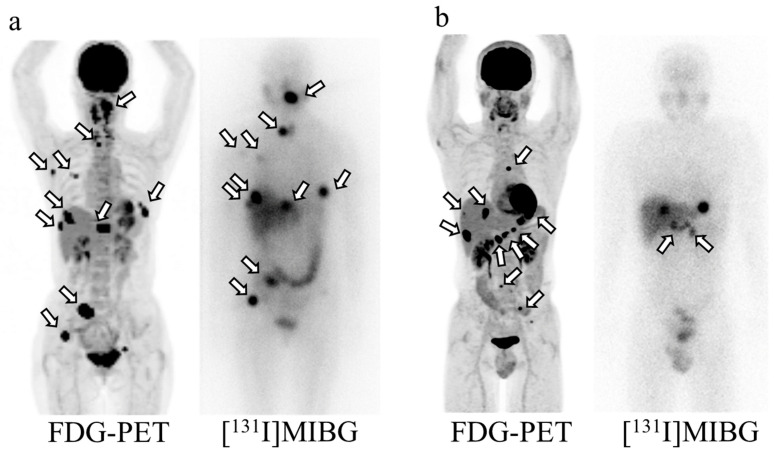
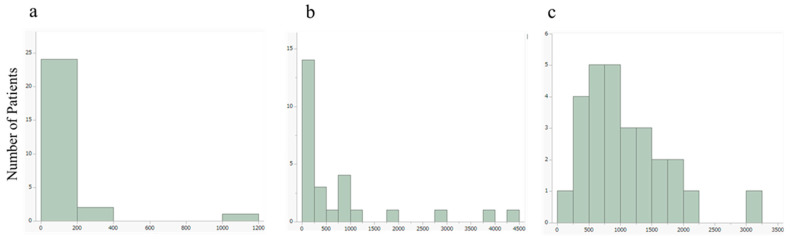
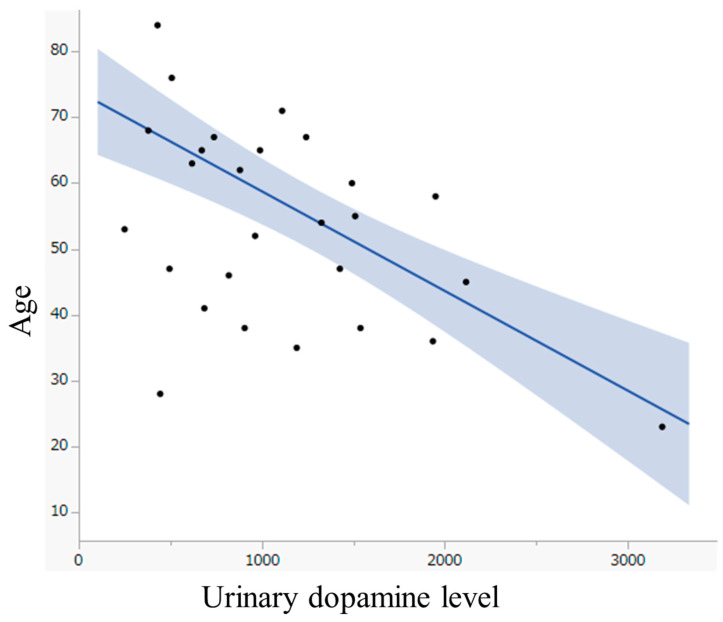
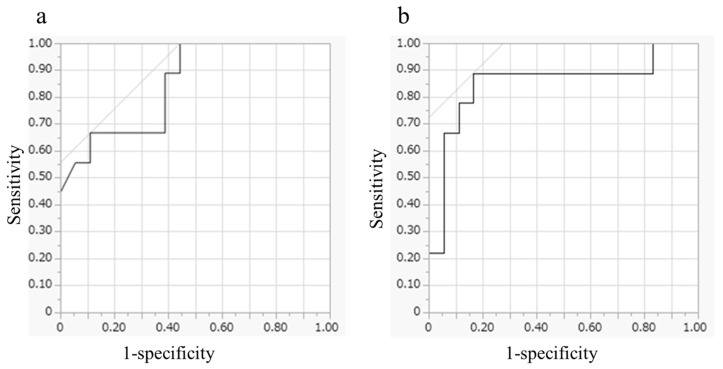
Background/Objectives: Pheochromocytomas and paragangliomas (PPGLs) are rare neuroendocrine tumors that produce catecholamines. Unresectable or metastatic PPGLs are treated with [131I]metaiodobenzylguanidine (MIBG), but MIBG avidity is often heterogeneous. Identifying predictive factors for non-avid lesions on scintigraphy is clinically important. The primary objective of this study was to investigate the relationship between MIBG avidity and catecholamine secretion patterns in patients with unresectable or metastatic PPGLs. Methods: This retrospective study included 27 patients treated with [131I]MIBG for unresectable/metastatic PPGLs between 2001 and 2024. Patients received a single intravenous dose of [131I]MIBG (5.5-7.4 GBq), with post-therapy scintigraphy performed 3-7 days later. Non-avid lesions were assessed by imaging and confirmed using CT, MRI, and FDG-PET. Clinical factors, including age, sex, prior treatments, metastasis sites, and urine catecholamines, were evaluated using univariate logistic analysis. Predictive factors were assessed via receiver operating characteristic curves. Results: Non-avid lesions were found in nine patients (33.3%). These patients were younger (median age 38 vs. 62.5 years) and had higher urine dopamine levels (median 1510 vs. 779 μg/day) than those without non-avid lesions. Younger age (odds ratio: 0.892, p < 0.01) and higher urinary dopamine levels (odds ratio: 1.003, p < 0.01) were significantly associated with non-avid lesions. All patients > 45 years with urinary dopamine < 1190 μg/day had no non-avid lesions, whereas patients < 45 years with urinary dopamine > 1190 μg/day had non-avid lesions. Conclusions: Age and urinary dopamine levels may predict non-avid lesions in unresectable/metastatic PPGLs, aiding treatment decisions for [131I]MIBG therapy. This article is a revised and expanded version of a paper entitled "Urine dopamine level and age can predict non-avid lesion on scintigraphy after I-131 MIBG treatment for unresectable/metastatic PPGL", which was presented at SNMMI 2024, Toronto, from 8 June to 11 June 2024.
Keywords: PPGL; [131I]MIBG therapy; urine catecholamine.
Conflict of interest statement
The authors have no potential conflicts of interest related to the content of this paper.
Figures
Similar articles
-
The Biochemical-Imaging Connection: Urinary Noradrenaline and Fluorodeoxyglucose-Positron Emission Tomography in Unresectable or Metastatic Pheochromocytomas and Paragangliomas.Diagnostics (Basel). 2025 May 22;15(11):1305. doi: 10.3390/diagnostics15111305. Diagnostics (Basel). 2025. PMID: 40506877 Free PMC article.
-
Predictive Factors of Early 18F-Fluorodeoxyglucose-Positron Emission Tomography Response to [131I] Metaiodobenzylguanidine Treatment for Unresectable or Metastatic Pheochromocytomas and Paragangliomas.Neuroendocrinology. 2024;114(9):816-826. doi: 10.1159/000534175. Epub 2023 Sep 19. Neuroendocrinology. 2024. PMID: 37725921 Free PMC article.
-
Prognostic value of [18F]FDG-PET prior to [131I]MIBG treatment for pheochromocytoma and paraganglioma (PPGL).Ann Nucl Med. 2023 Jan;37(1):10-17. doi: 10.1007/s12149-022-01798-6. Epub 2022 Oct 27. Ann Nucl Med. 2023. PMID: 36301465
-
Detection and treatment of pheochromocytomas and paragangliomas: current standing of MIBG scintigraphy and future role of PET imaging.Q J Nucl Med Mol Imaging. 2008 Dec;52(4):419-29. Q J Nucl Med Mol Imaging. 2008. PMID: 19088695 Review.
-
Metastatic Pheochromocytomas and Abdominal Paragangliomas.J Clin Endocrinol Metab. 2021 Apr 23;106(5):e1937-e1952. doi: 10.1210/clinem/dgaa982. J Clin Endocrinol Metab. 2021. PMID: 33462603 Free PMC article. Review.
Cited by
-
The Biochemical-Imaging Connection: Urinary Noradrenaline and Fluorodeoxyglucose-Positron Emission Tomography in Unresectable or Metastatic Pheochromocytomas and Paragangliomas.Diagnostics (Basel). 2025 May 22;15(11):1305. doi: 10.3390/diagnostics15111305. Diagnostics (Basel). 2025. PMID: 40506877 Free PMC article.
References
-
- Berends A.M.A., Buitenwerf E., de Krijger R.R., Veeger N.J.G.M., van der Horst-Schrivers A.N.A., Links T.P., Kerstens M.N. Incidence of pheochromocytoma and sympathetic paraganglioma in the Netherlands: A nationwide study and systematic review. Eur. J. Intern. Med. 2018;51:68–73. doi: 10.1016/j.ejim.2018.01.015. - DOI - PubMed
-
- Choi Y.M., Sung T.-Y., Kim W.G., Lee J.J., Ryu J.-S., Kim T.Y., Kim W.B., Hong S.J., Song D.E., Shong Y.K. Clinical course and prognostic factors in patients with malignant pheochromocytoma and paraganglioma: A single institution experience. J. Surg. Oncol. 2015;112:815–821. doi: 10.1002/jso.24063. - DOI - PubMed
LinkOut - more resources
Full Text Sources
