

Effect of Current-Season-Only Versus Continuous Two-Season Influenza Vaccination on Mortality in Older Adults: A Propensity-Score-Matched Retrospective Cohort Study
- PMID: 40006711
- PMCID: PMC11860298
- DOI: 10.3390/vaccines13020164
Effect of Current-Season-Only Versus Continuous Two-Season Influenza Vaccination on Mortality in Older Adults: A Propensity-Score-Matched Retrospective Cohort Study
Abstract
Background/objectives: This study evaluated the impact of influenza vaccination on mortality using real-world data and compared the effect of current-season-only vaccination versus continuous two-season vaccination.
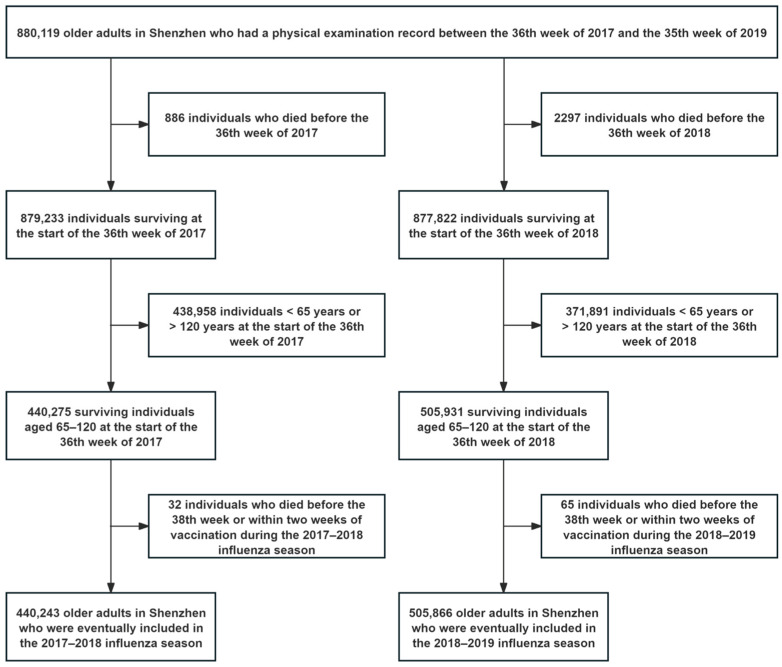
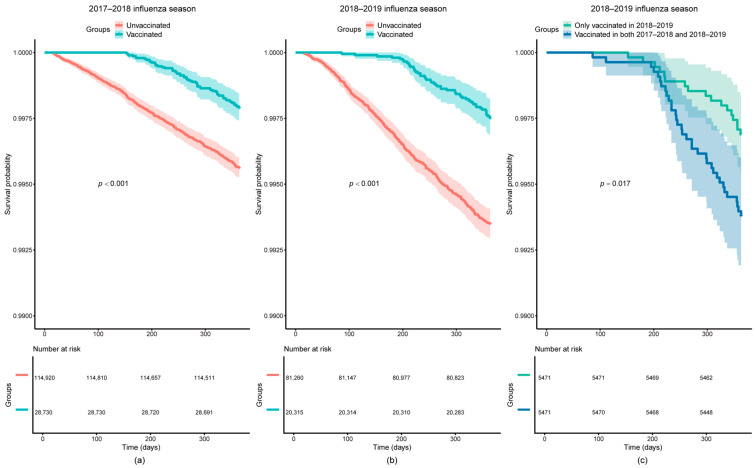
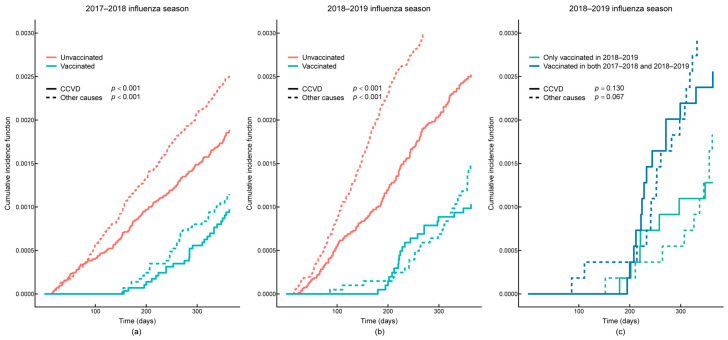
Methods: The 2017-2019 data from the Center for Disease Control and Prevention of Shenzhen, Guangdong, China, included 880,119 individuals aged ≥65 years. The participants were divided into vaccinated and unvaccinated groups and matched using propensity scores with a 1:4 nearest-neighbor approach. Vaccinated individuals were further divided into current-season-only and continuous two-season vaccination groups, matched 1:1. Cox's multivariable proportional hazards regression models were used to assess the effect of vaccination on all-cause mortality, with Firth's penalized likelihood method applied to correct for a few events. The Fine-Gray competing risk models were used to assess the effect of vaccination on cardio-cerebral vascular disease (CCVD) mortality. Sensitivity analyses, including caliper matching, a nested case-control design, and Poisson's regression, were performed to test the robustness of the results.
Results: Influenza vaccination reduced all-cause mortality by 39% (HR = 0.61, 95% CI: 0.47-0.80) and 55% (HR = 0.45, 95% CI: 0.33-0.60) in 2017-2018 and 2018-2019, respectively. Current-season-only vaccination showed stronger protective effects than continuous two-season vaccination (HR = 0.56, 95% CI: 0.31-0.99). Influenza vaccination reduced CCVD mortality by 46% (HR = 0.54, 95% CI: 0.34-0.84) in 2018-2019. The results were consistent across the sensitivity analyses.
Conclusions: Influenza vaccination was associated with a reduced risk of all-cause and CCVD mortality in older adults, underscoring the importance of routine influenza vaccination in older populations. Stronger effects were observed for current-season-only vaccination, warranting further research to confirm the association and explore mechanisms.
Keywords: cardio-cerebral vascular diseases; influenza vaccination; mortality; older adults; survival analysis.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the study design, data analyses, manuscript writing, or in the decision to publish the results.
Figures
Similar articles
-
Influenza vaccination and mortality among adults with heart failure in an integrated healthcare delivery system, 2009-2018.J Gen Intern Med. 2022 Aug;37(10):2405-2412. doi: 10.1007/s11606-021-07068-x. Epub 2021 Aug 11. J Gen Intern Med. 2022. PMID: 34379280 Free PMC article.
-
Insights into the protective effects of influenza vaccination: More hospitalizations but lower follow-up mortality during the 2014/15 influenza season in a Swiss cohort.Vaccine. 2020 Jul 14;38(33):5187-5193. doi: 10.1016/j.vaccine.2020.06.019. Epub 2020 Jun 19. Vaccine. 2020. PMID: 32571721
-
Influenza vaccination and 1-year risk of myocardial infarction, stroke, heart failure, pneumonia, and mortality among intensive care unit survivors aged 65 years or older: a nationwide population-based cohort study.Intensive Care Med. 2019 Jul;45(7):957-967. doi: 10.1007/s00134-019-05648-4. Epub 2019 Jun 11. Intensive Care Med. 2019. PMID: 31187170
-
The impact of repeated vaccination on influenza vaccine effectiveness: a systematic review and meta-analysis.BMC Med. 2019 Jan 10;17(1):9. doi: 10.1186/s12916-018-1239-8. BMC Med. 2019. PMID: 30626399 Free PMC article.
-
Cardioprotective effects of influenza vaccination among patients with established cardiovascular disease or at high cardiovascular risk: a systematic review and meta-analysis.Eur J Prev Cardiol. 2022 Oct 20;29(14):1881-1892. doi: 10.1093/eurjpc/zwac152. Eur J Prev Cardiol. 2022. PMID: 35857821
References
-
- World Health Organization Influenza (Seasonal) [(accessed on 31 December 2024)]. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal)
-
- World Health Organization Vaccines Against Influenza: WHO Position Paper—May 2022. [(accessed on 31 December 2024)]. Available online: https://www.who.int/publications/i/item/who-wer9719.
Grants and funding
LinkOut - more resources
Full Text Sources
