

Predictive Effect of Atypical Right Bundle-Branch Block on In-Hospital Sudden Cardiac Death and Cardiac Rupture and Long-Term Prognosis in Patients With Acute Myocardial Infarction Who Underwent Percutaneous Coronary Intervention
- PMID: 40008523
- PMCID: PMC12132683
- DOI: 10.1161/JAHA.124.038344
Predictive Effect of Atypical Right Bundle-Branch Block on In-Hospital Sudden Cardiac Death and Cardiac Rupture and Long-Term Prognosis in Patients With Acute Myocardial Infarction Who Underwent Percutaneous Coronary Intervention
Abstract
Background: A study was conducted to explore the predictive effect of atypical right bundle-branch blocks (ARBBB) on in-hospital sudden cardiac death (SCD), cardiac rupture (CR), and long-term prognosis in patients with acute myocardial infarction undergoing percutaneous coronary intervention with a drug-eluting stent.
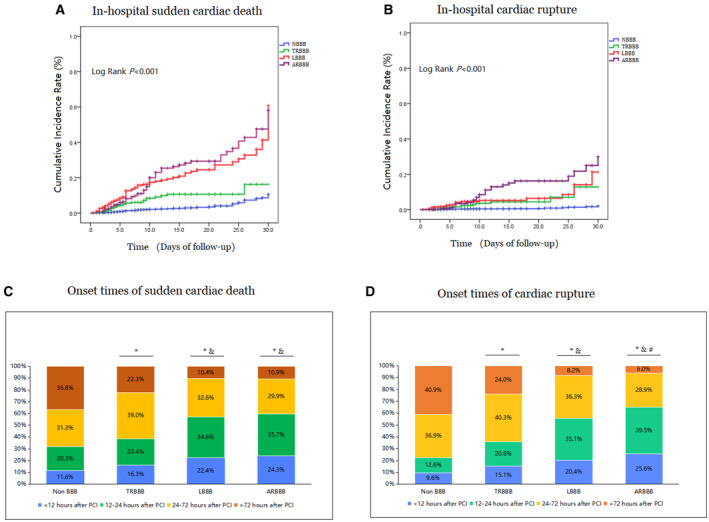
Methods and results: A total of 13 886 patients with first-episode acute myocardial infarction who underwent percutaneous coronary intervention with a drug-eluting stent at 3 centers from January 2017 to January 2022 were included in this retrospective study. Patients were categorized into 4 groups: ARBBB (n=348), typical right BBB (n=374), left BBB (n=366), and non-BBB (n=12 798). The primary end points were in-hospital SCD and CR, the secondary end points were 2-year major adverse cardiovascular and cerebrovascular events. During the in-hospital observation period, 334 patients (2.4%) experienced SCD, with 98 (0.7%) attributed to CR. The incidences of in-hospital SCD and CR in the group with ARBBB were significantly higher than those in the other 3 groups (ARBBB versus left BBB versus typical right BBB versus non-BBB: SCD, 10.6% versus 5.7% versus 4.3% versus 2.0%, P=0.001; CR, 5.7% versus 2.7% versus 1.3% versus 0.5%, P<0.001). ARBBB was a statistically significant predictor of in-hospital SCD (hazard ratio [HR], 2.45 [95% CI, 1.65-4.78], P<0.001) and CR (HR, 3.32 [95% CI, 1.77-7.74], P<0.001). ARBBB could also predicted the 2-year major adverse cardiovascular and cerebrovascular events (HR, 2.99 [95% CI, 1.65-5.53], P<0.001).
Conclusions: ARBBB is a predictor of in-hospital SCD, CR, and 2-year major adverse cardiovascular and cerebrovascular events in patients with first-episode acute myocardial infarction undergoing percutaneous coronary intervention with a drug-eluting stent.
Keywords: MACCE; acute myocardial infarction; atypical right bundle‐branch block; cardiac rupture; percutaneous coronary intervention; sudden cardiac death.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
